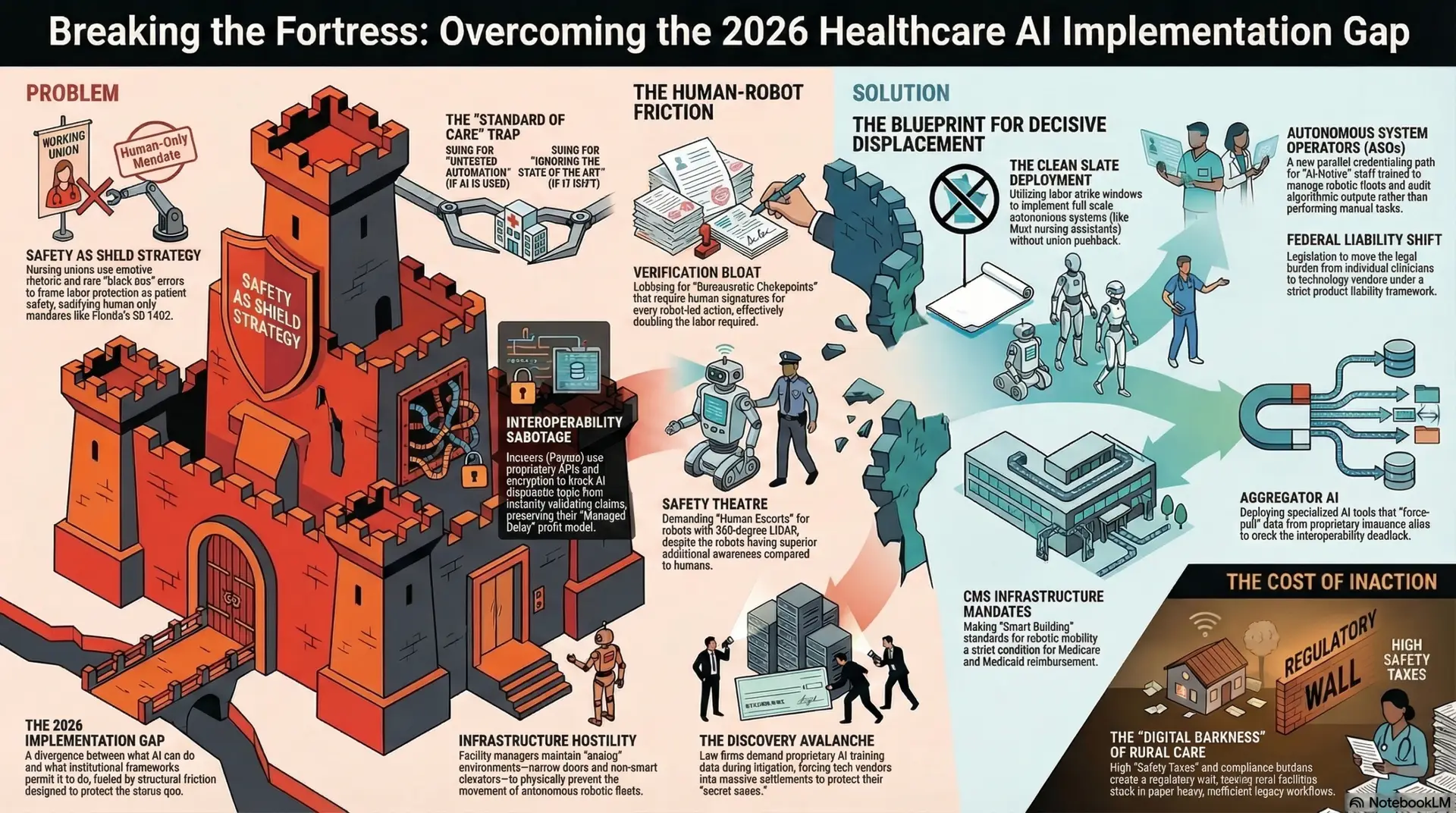
The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier, RN / AI Nurse Hub
Date: March 7, 2026
Abstract
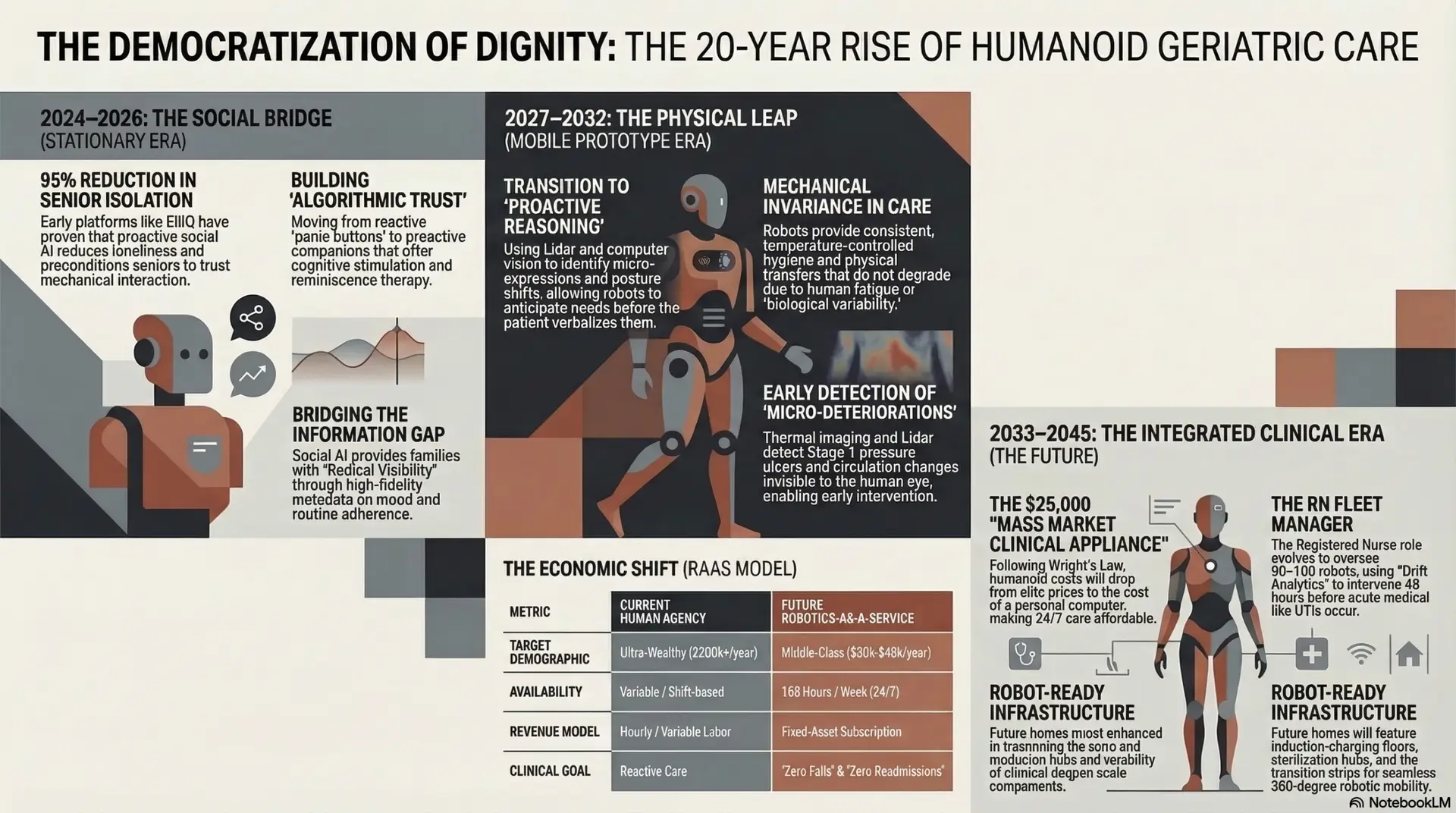
The home care industry is currently entering its “iPhone Moment”—a pivotal transition where “general purpose” humanoid hardware is poised to replace single-use medical devices and fragmented human labor. This article explores the 20-year trajectory of geriatric robotics, tracing the evolution from stationary social AI companions to fully embodied, mobile caregivers. By analyzing the psychological preconditioning provided by platforms like ElliQ, the clinical superiority of mechanical invariance in Activities of Daily Living (ADLs), and the economic democratization of care through Robotics-as-a-Service (RaaS) models, this paper argues that humanoid robotics under the oversight of Registered Nurse (RN) Fleet Managers represent the only scalable solution to the global labor deficit. For the healthcare entrepreneur, this transition offers a path to providing 24/7 high-fidelity care to middle-income populations previously excluded from the elite agency market, effectively closing the “Care Desert” that currently plagues the American aging landscape. This expansion explores the nuances of algorithmic trust, the physiological mechanics of proactive reasoning, and the behavioral economics of mass-market robotic adoption.
I. Introduction: The Great Convergence
In 2007, the introduction of the smartphone fundamentally rearchitected global communication and commerce by consolidating multiple devices—phones, cameras, music players, and computers—into a single, general-purpose platform. In 2026, we find ourselves at a similar precipice in healthcare. We are witnessing the “Great Convergence” of large language models (LLMs), high-torque robotic actuators, and a desperate socioeconomic need. The American home care industry faces a projected shortfall of over 151,000 paid caregivers by 2030 (PHI, 2024), a gap that traditional recruitment and wage-incentive strategies have failed to close.
This labor vacuum acts as a catalyst for “Embodied AI”—the transition of artificial intelligence from the digital screen to the physical world. Unlike previous generations of “service robots” that were designed for single tasks (e.g., automated vacuuming or pill dispensing), the emerging humanoid era is defined by versatility. A single humanoid unit can transition from a laundry task to a complex patient transfer, and then to a diagnostic skin assessment. The evolution of geriatric care is moving through a predictable arc: from cognitive support to physical surrogacy. This democratization of safety ensures that 24/7 clinical monitoring and assistance are no longer reserved for the ultra-wealthy who can afford 24/7 human agencies, but become a baseline utility for the aging middle class who currently fall into a “Care Gap”—too wealthy for Medicaid support but too poor for private-duty nursing.
II. The Social Bridge: Cognitive Wellness and the Family Trust Architecture
The success of humanoid robotics depends less on mechanical engineering and more on psychological acceptance. The “Uncanny Valley”—the sense of unease caused by robots that appear almost, but not quite, human—remains a significant hurdle; however, platforms like Intuition Robotics’ ElliQ have served as the essential “Social Bridge.” By early 2024, data revealed that proactive social AI could reduce feelings of isolation in seniors by 95% (Intuition Robotics, 2024).
The Psychological Preconditioning of the Elder For the senior, the social bridge functions as a vital training ground for “Algorithmic Trust.” Traditional geriatric technology, such as “panic buttons” or passive motion sensors, are inherently reactive and stigmatizing, often signaling a loss of autonomy and the beginning of institutionalization. Conversely, proactive AI initiates interaction, offering reminiscence therapy, cognitive stimulation, and social connectivity. This interaction preconditions the user to view the machine not as a sterile medical tool, but as a reliable, supportive presence.
As these desktop units evolve into mobile humanoids, the senior has already overcome the psychological barrier of “interacting with a machine.” This transition reduces the cortisol spikes typically associated with unfamiliar human caregivers entering the private sanctity of the home. The resulting psychological safety is a critical clinical outcome; when a patient feels safe and understood by their primary caregiver—mechanical or otherwise—rates of dementia-related agitation, sundowning, and depression plummet. The robot becomes a “known entity,” providing a level of emotional stability that a rotating staff of human aides cannot replicate.
The Trust Architecture for the Family For the family, the social bridge provides “Radical Visibility.” The primary stressor for the “sandwich generation”—those caring for both children and aging parents—is the lack of real-time, objective data regarding their loved one’s safety. Social AI platforms bridge this “Information Gap” by providing high-fidelity metadata regarding the patient’s mood, cognitive engagement, and adherence to routines. This visibility mitigates the pervasive “caregiver guilt” that often leads to family burnout. The social bridge is effectively a trust-building phase that secures the family’s investment, proving that digital oversight can be as empathetic and reliable as a human pulse.
III. The Great Physical Leap: Proactive Reasoning and Physiological Comfort
The transition from desktop companions to mobile humanoids (e.g., Fourier GR-1, 1X Neo, and Tesla Optimus) represents the end of the “High-Mass Transfer” crisis. For nurses and entrepreneurs, the clinical benefits of “Mechanical Invariance” (performance that does not degrade with time) and “Proactive Reasoning” lead to a quantifiable reduction in patient discomfort.
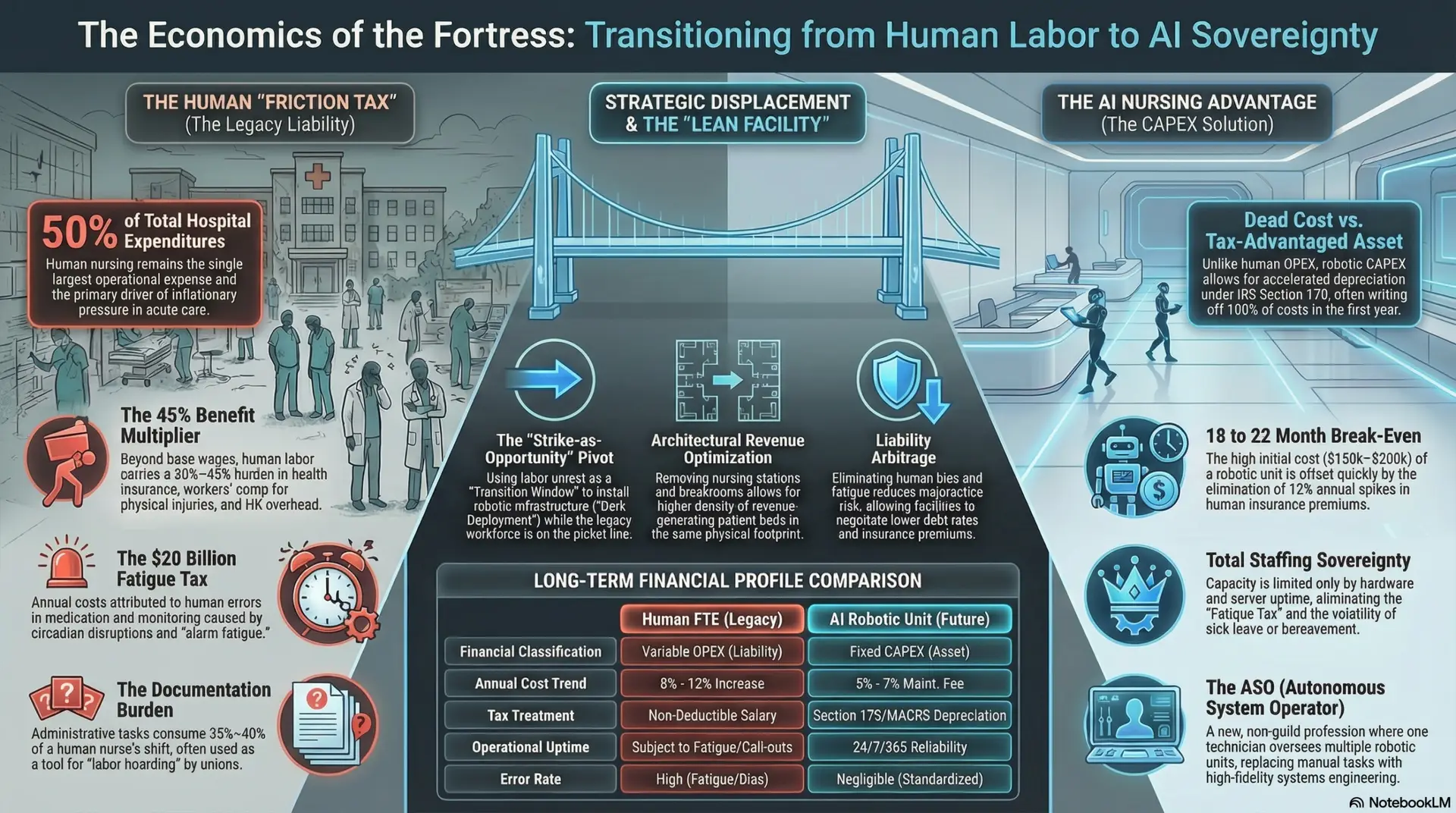
IV. The Economics of Democratization: Entrepreneurial Opportunity
The democratization of care follows Wright’s Law: as cumulative production doubles, costs drop at a consistent percentage. We are moving from the era of $150,000 elite prototypes to $25,000 “Mass Market Clinical Appliances” by the mid-2030s, mirroring the price drop of the early personal computer.
The Entrepreneur’s Opportunity: Bridging the “Middle-Class Gap” The current home care market is bifurcated: high-net-worth individuals pay $200k+ annually for 24/7 human care, while low-income individuals rely on strained Medicaid programs. The middle class—those with retirement savings but finite assets—is currently stranded in a “Care Desert.” For the entrepreneur, humanoid robotics represent a disruptive market entry into this massive, underserved segment.
By utilizing a Robotics-as-a-Service (RaaS) model, an agency can provide 24/7 clinical safety for approximately $2,500 to $4,000 per month. This model transforms home care from a “variable-cost human liability” into a “fixed-asset clinical utility.” The business owner can capitalize on this by:
V. The Human-Robot Synergy: The RN as Fleet Manager
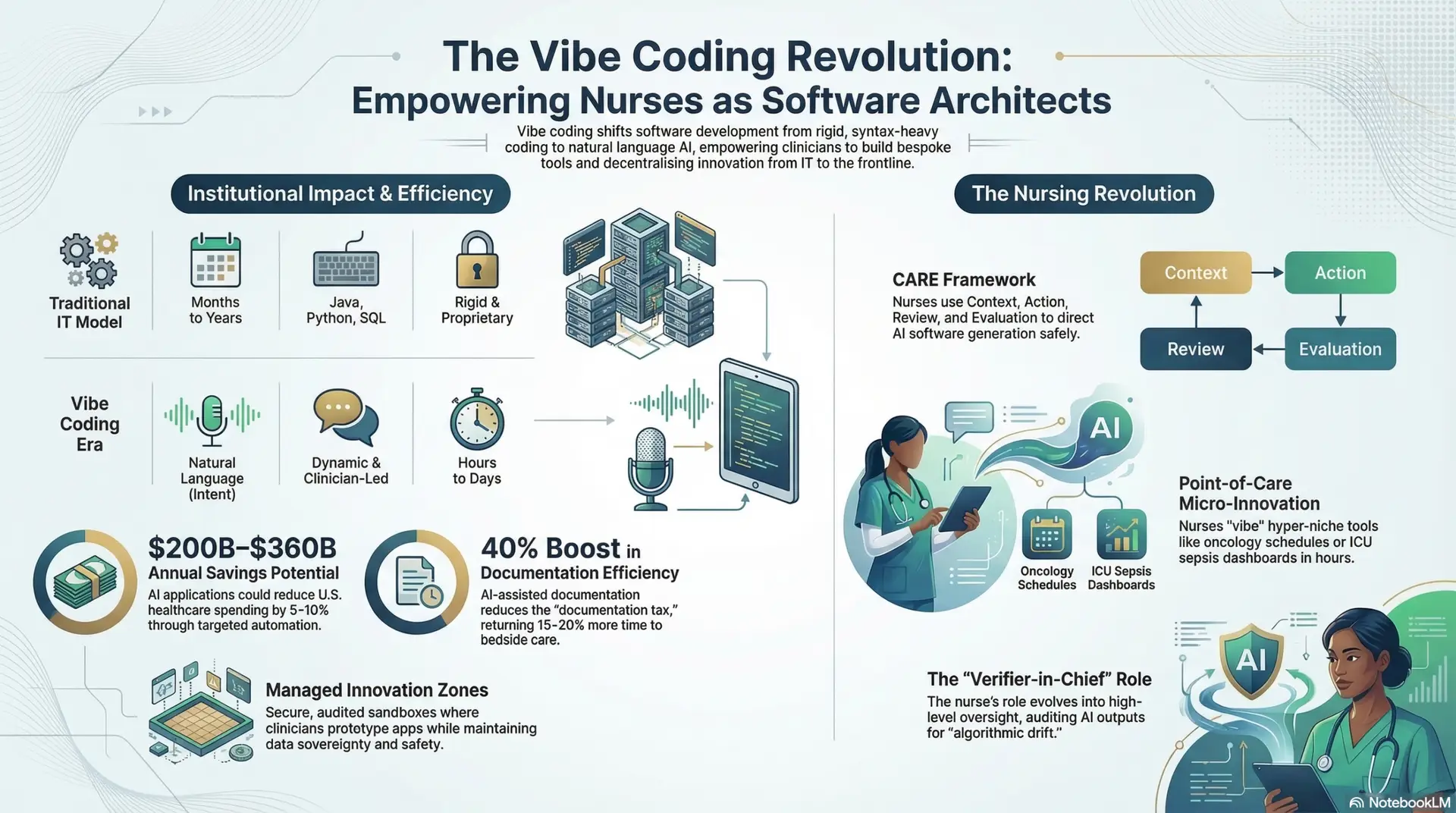
The role of the Registered Nurse is undergoing a professional metamorphosis from “Bedside Tasking” to Clinical Systems Architecture. In the 20-year horizon, the RN functions as a Fleet Manager, overseeing a regional hub of humanoid units.
This model utilizes Digital Delegation, a framework where the RN “signs off” on assessments and physical tasks performed by the robot surrogate. By intervening based on “Drift Analytics” (identifying a 5% decline in gait before a fall occurs), the RN Fleet Manager effectively eliminates unnecessary hospital readmissions—the most expensive failure in the current healthcare system. The nurse moves from being a manual laborer to being the ultimate guarantor of safety and the clinical decision-maker for a large-scale population. This shift not only protects the nurse from physical injury but also elevates the profession to a role of data-driven leadership.
VI. Infrastructure: Now, Emerging, and Probable Future
To realize this vision, the infrastructure of the American home must evolve. Entrepreneurs and developers must anticipate these stages of “Robot-Ready” environments:
VII. Conclusion: The Inevitability of Reliable Care
The transition to humanoid robotics in geriatric care is not merely a technological achievement; it is a democratization of dignity. By bridging the gap from desktop chatbots to embodied mobile caregivers, we are creating a future where “Aging in Place” is no longer a privilege of the wealthy or a gamble for the poor.
Under the oversight of the RN Fleet Manager, the humanoid robot becomes the ultimate guarantor of safety and physical comfort, ensuring that the sunset years of our population are defined by reliability, precision, and the highest standards of clinical care. For the entrepreneur, the path is clear: those who build the infrastructure for this “Integrity Dividend” now will lead the most significant shift in healthcare delivery since the industrial revolution. The era of manual, variable care is ending; the era of automated autonomy and democratic dignity is beginning.
References
Mullainathan, S., & Shafir, E. (2024).Scarcity: Why
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026