The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier, RN / AI Nurse Hub
Date: March 7, 2026
Abstract
The American home care industry is currently navigating a state of terminal economic failure. Traditional discourse often frames the rise of humanoid robotics as a threat to human employment; however, a rigorous analysis of labor data and economic theory reveals a “Care Vacuum”—a massive, pre-existing void where human labor is no longer available, affordable, or reliable. This article, the final in a four-part series, examines the “Direct Care Trap” that renders human-led agencies mathematically unsustainable. By synthesizing Baumol’s Cost Disease with the clinical costs of institutional memory loss, this paper argues that humanoid robotics, governed by Registered Nurse (RN) Systems Architects and Regional Hub Managers, are the only viable mechanism to restore a “Safety Floor” of care. The transition to automated autonomy is not a choice between humans and machines, but between a state of systemic neglect and a future of democratized, reliable dignity. This framework provides the economic and professional blueprint for a new era of nurse-led technological intervention in the domestic sphere.
I. Introduction: Beyond the “Shortage” Narrative
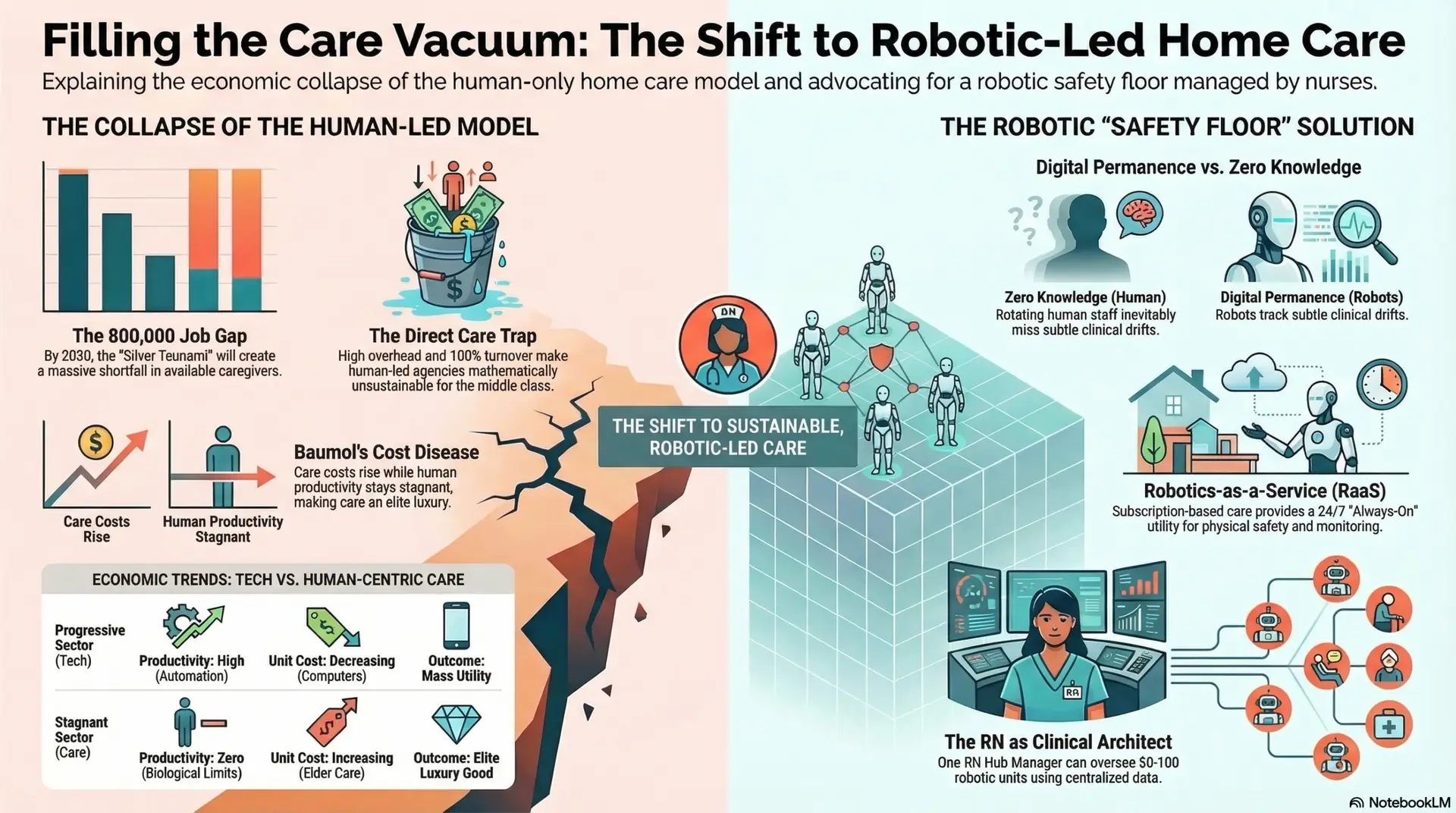
The prevailing narrative in geriatric care is one of a “labor shortage.” This terminology is fundamentally flawed, as it implies a temporary dip in supply that can be corrected through traditional recruitment or wage incentives. In reality, we are witnessing a “Care Vacuum”—a structural collapse driven by a projected shortfall of over 800,000 annual job openings by 2030 (PHI, 2024). This is not a cyclical fluctuation; it is a permanent demographic realignment.
This vacuum is the result of a “Silver Tsunami” colliding with a “Labor Drought.” The caregiver support ratio—the number of available workers aged 45-64 for every person over 80—is expected to drop from 7:1 in 2010 to 4:1 by 2030. When this demographic reality is coupled with the fact that the “sandwich generation” is increasingly unable to provide unpaid familial care due to their own economic pressures, the result is a total systemic failure. While human presence remains the clinical ideal, the current labor market can no longer guarantee even a baseline of physical safety or medication adherence. Robotics must now provide the “floor” of consistency that an overextended and biologically limited workforce cannot sustain. The vacuum is already here; millions of seniors are currently living in “Care Deserts” where services are unavailable at any price point.
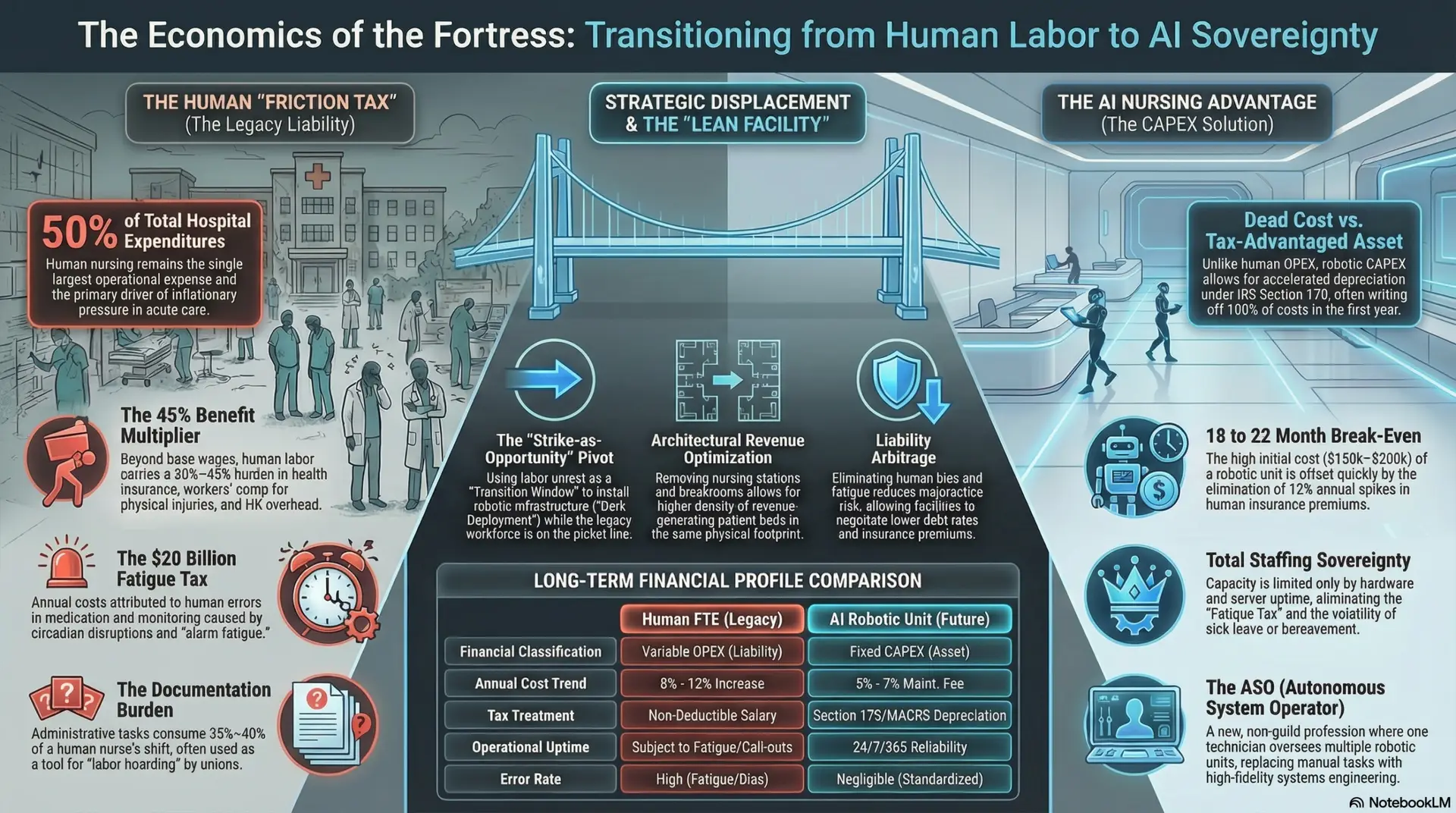
II. The Wage-Gap Paradox and the “Direct Care Trap”
For the healthcare entrepreneur, the “Direct Care Trap” is the primary barrier to business viability. Currently, the industry standard involves an agency billing rate of approximately $35 per hour, while the direct care worker receives a take-home wage of roughly $16 per hour. This $19 “spread” is frequently misunderstood by the public as “corporate greed,” yet a granular Break-Even Analysis reveals the terminal math of the human-led model:
The Trap Defined: If an agency attempts to pay a living wage of $25/hr to stabilize its workforce, the billable rate must climb to $65–$75/hr to maintain even a meager 5% net margin. This price point effectively bankrupts the middle class, forcing seniors into premature institutionalization in Medicaid-funded facilities. The entrepreneur is thus trapped in a model where they cannot pay enough to keep workers, yet cannot charge enough to remain solvent. The vacuum is formed by this economic impossibility.
III. Baumol’s Cost Disease: The Productivity Dead-End
The economic failure of home care is fundamentally explained by Baumol’s Cost Disease. This theory posits that in “labor-intensive” sectors where productivity does not increase (such as human caregiving), costs will inevitably rise to keep pace with wages in “progressive” sectors (such as tech or manufacturing) where technology does increase productivity. This is known as “unbalanced growth.”
In manufacturing, a worker can produce 100 times more “widgets” per hour than they did 50 years ago due to automation. In home care, it takes a human the same amount of time to perform a bed bath or assist with a transfer today as it did in 1950. Humans do not scale. This creates a Productivity/Price Divergence:
| Feature | Progressive Sector (Tech/Mfg) | Stagnant Sector (Human Home Care) |
| Productivity Growth | High (Automation/Efficiency) | Zero (Biological Limitation) |
| Wage Trend | Rising (due to productivity) | Must rise (to compete for labor) |
| Unit Cost | Decreasing (e.g., Computers) | Increasing (e.g., Elder Care) |
| Outcome | Becomes a Mass Utility | Becomes an Elite Luxury Good |
As the “Progressive Sectors” drive up the cost of labor generally, the “Stagnant Sector” of home care must pay more to attract workers, but because there is no corresponding increase in efficiency, the cost is passed directly to the consumer. Humanoid robotics represent the only Productivity Hedge available. By deploying a robotic surrogate that can work 168 hours a week without fatigue, we finally introduce “Progressive Sector” economics into the geriatric home, making care a scalable utility rather than an expensive, limited-resource service.
IV. The Churn Trap: “Zero Knowledge” vs. Digital Permanence
The 100%+ turnover rate in home care creates a “Revolving Door” that is clinically dangerous. When a patient deals with 3-5 different strangers in a single week, Institutional Memory—the accumulation of subtle, individualized patient knowledge—is lost.
V. The Scalability Crisis: Comparative Sector Analysis
Home care is currently losing the war for labor to the retail, hospitality, and logistics sectors, creating a “Human Choice Friction” that favors lower-stress environments.
VI. The Utility of Care Model: The Saving Grace
We must shift from viewing home care as an “Intermittent Transactional Service” to an “Always-On Utility.”
VII. Final Call to Action: Filling the Void
The final ethical question for healthcare entrepreneurs and nursing leaders is no longer “Is it cold to use a robot?” but “Is it negligent to leave a senior alone in a vacuum?” We must shift our focus from “replacing humans” to “filling the void” where humans have already departed.
The era of automated autonomy is the only path to democratic, safe, and reliable dignity. By embracing the “Integrity Dividend” of humanoid robotics, we empower nurses to work as the ultimate Clinical Architects of the home, guaranteeing that no senior is ever left to face the sunset of their life in an empty, unmonitored house. The vacuum is real; it is our professional and moral duty to fill it with reliable, robotic permanence. We are not automating care; we are automating the physical labor so that care can finally be delivered with the precision and frequency it requires.
References
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026