The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier, RN AI Nurse Hub
Date: March 7, 2026
Abstract
The modern home care industry operates within a “Domestic Black Box,” a clinical environment characterized by high-risk tasks performed in total isolation with minimal oversight. While traditional discourse prioritizes “human-centric” care, current data reveals a systemic integrity vacuum defined by high turnover, financial scarcity among caregivers, and significant rates of undetected elder abuse. This article argues that the integration of humanoid robotics, overseen by Registered Nurse (RN) Clinical Forensic Auditors, provides a necessary “Safety Floor” for an aging population. By analyzing the socioeconomic volatility of the low-wage workforce and the “mechanical invariance” of embodied AI, this paper posits that reliability is the highest form of clinical ethics. The transition to robotic surrogacy does not replace the human element but rather secures it, providing a transparent, auditable trail of care that protects the most vulnerable members of society from the crimes of opportunity inherent in unvetted domestic labor. This “Integrity Dividend” serves as a new gold standard for quality assurance in the domestic sphere.
I. Introduction: The “Safety Mirage” of Unvetted Care
The American home care sector is currently sustained by a “Safety Mirage”—a collective, often desperate belief that the presence of a human caregiver in the home inherently guarantees safety and companionship. In reality, the domestic environment is the most unregulated and opaque clinical setting in the healthcare continuum. Unlike the hospital or long-term care facility, which benefit from the “witness effect”—where peer observation and supervisory oversight provide a natural check against negligence—the home is a silo.
This lack of visibility has facilitated the proliferation of the “Gray Market,” an unregulated shadow economy of “find-a-caregiver” platforms and word-of-mouth hiring that bypasses formal clinical vetting. Driven by a massive labor vacuum, families are often forced into a “Vetting Gap,” where they prioritize immediate availability over verifiable security credentials. This results in individuals with unverified backgrounds gaining unsupervised access to the physical and financial assets of vulnerable seniors.
The consequences of this gap are often catastrophic but hidden. The theoretical “2024 Midwest HHA Multi-Agency Crisis” serves as a stark reminder; in that instance, a lack of systemic oversight allowed for months of undetected neglect and medication diversion across three states before a clinical outcome forced a post-mortem audit. In contrast, early robotic pilot programs in 2025 demonstrated that embodied AI provides a persistent, objective presence. By removing the “Black Box” effect, robotics transform the home into a transparent clinical environment where the “witness effect” is digitally architected rather than humanly dependent.
II. The Taboo: Breaking the Silence on Elder Abuse
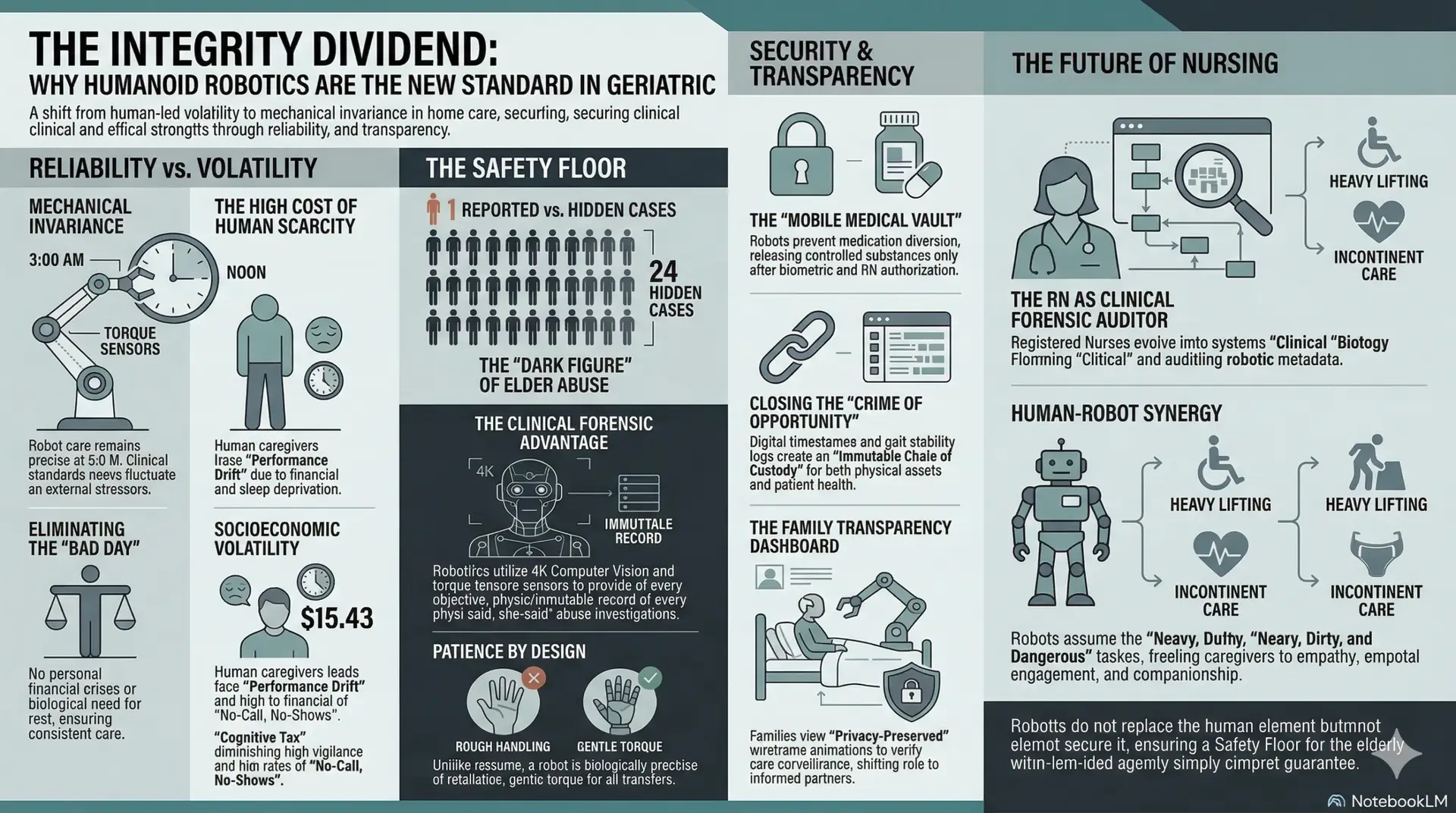
Elder abuse remains a silent epidemic in the domestic sphere, often shielded by the very “human-centric” sentimentality used to market home care services. According to the National Center on Elder Abuse (NCEA, 2024) and recent KFF data (2025), approximately one in ten older adults experience some form of mistreatment. However, these figures represent only the visible portion of a much larger crisis. The NCEA describes a “Dark Figure of Crime,” estimating that for every one case of abuse reported to authorities, approximately 24 cases remain hidden.
The modalities of abuse at the hands of domestic caregivers are diverse, insidious, and often subtle:
Humanoid robotics, equipped with Lidar, 4K Computer Vision, and high-frequency torque sensors, offer a “Clinical Forensic Advantage.” By providing an objective, immutable record of every physical interaction, robotics eliminate the “he-said, she-said” nature of abuse investigations. A robot is biologically incapable of frustration or retaliation. Its “mechanical patience” ensures that a transfer at 3:00 AM for a sundowning patient is executed with the exact same precise, gentle torque and vocal de-escalation as a routine check-in at noon.
III. Financial Exploitation: Closing the “Crime of Opportunity”
The home is not just a clinical site; it is a repository of a lifetime of financial assets, making it a prime location for “crimes of opportunity.” Financial exploitation in home care ranges from simple theft of jewelry to complex identity theft, property scams, and the pervasive issue of medication diversion—specifically of high-value opioids.
Traditional agencies struggle to police these incidents because they rely on human honesty in a low-wage, high-stress environment. A robotic system, however, provides a radical departure from this risk. Every interaction within the home is timestamped and logged. Furthermore, the robot’s internal storage can be configured as a “mobile medical vault” for high-risk medications. In this model, the robot only dispenses controlled substances after receiving biometric authorization from a remote RN and verifying the patient’s identity via facial recognition.
This creates an “Immutable Chain of Custody” for both physical and financial assets. For high-net-worth families and fiduciaries, this level of auditability is not just a feature; it is the “Integrity Dividend”—a primary differentiator that provides peace of mind that human-led agencies simply cannot guarantee.
IV. The “Family Transparency Dashboard”: Promoting Radical Trust
To bridge the “Guilt Gap” felt by adult children who cannot be physically present due to geographic or professional constraints, the future of healthcare must prioritize visibility. The “Family Transparency Dashboard” provides a revolutionary user interface that allows authorized family members to view real-time “Integrity Scores” and care metadata.
Crucially, this is not invasive video surveillance, which many patients find undignified. Instead, the dashboard utilizes “Privacy-Preserved Visualization”—wireframe animations derived from sensor data that verify care tasks have been completed. A family member can log in and see a digital representation of their parent being successfully transferred, a log of their nutritional and fluid intake, and an objective score of their gait stability. This visibility transforms the “Black Box” into a space of “Radical Trust.” It shifts the family’s role from anxious investigators to informed partners in the care process, providing definitive, data-driven proof of care quality.
V. The Reliability Factor: Mechanical Invariance vs. Socioeconomic Volatility
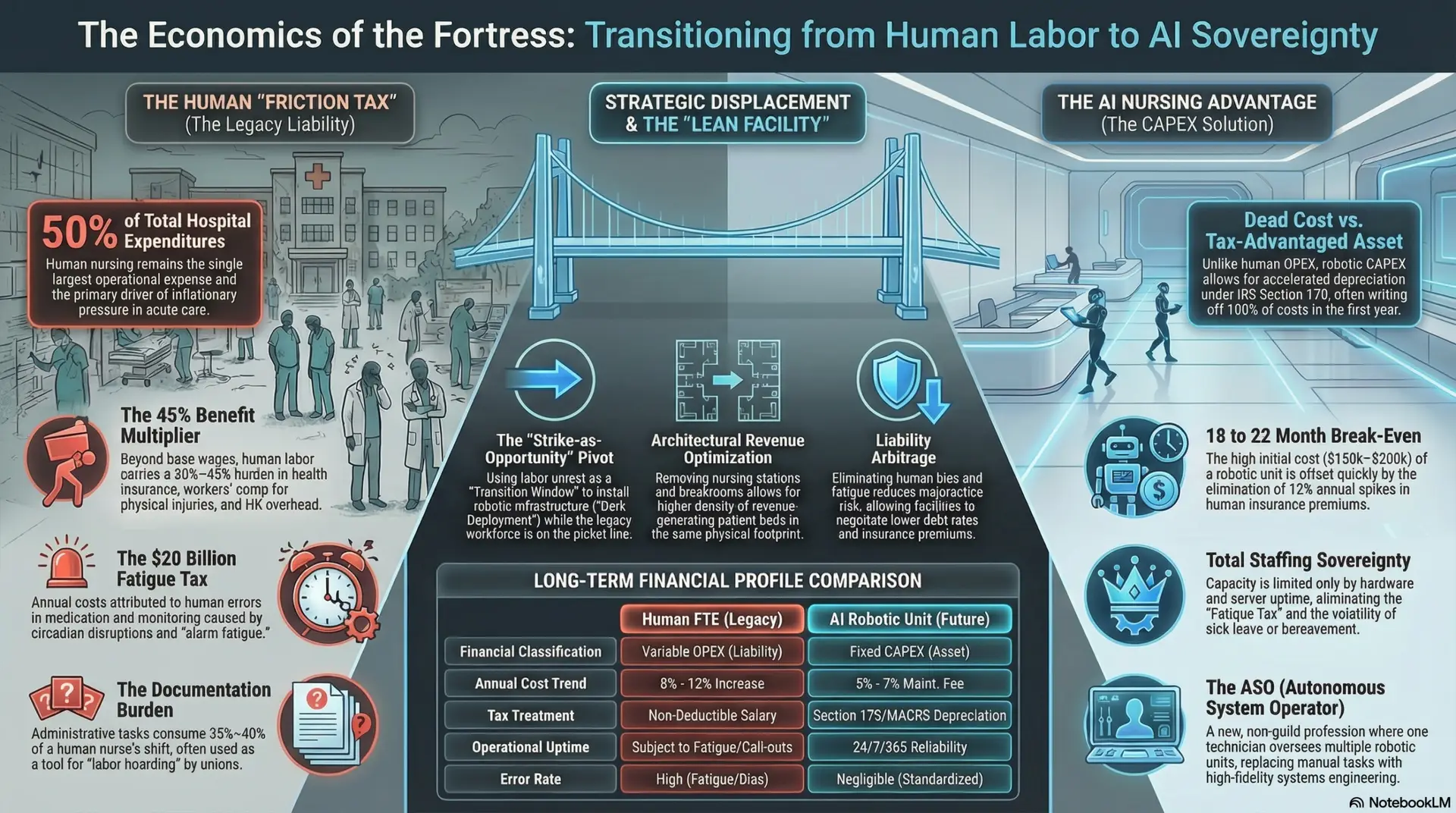
The most significant, yet least discussed, risk in home care is the socioeconomic volatility of the human workforce. The direct care workforce currently earns a median wage of $15.43 (PHI, 2024), a level of pay that keeps many workers in a state of chronic “Scarcity” (Mullainathan & Shafir, 2024).
This financial scarcity imposes a heavy “Cognitive Tax” on the caregiver. When a worker is worried about an impending eviction, a car breakdown, or a childcare crisis, their “bandwidth” for clinical vigilance is severely diminished. Many aides work 60+ hours across multiple agencies just to reach a living wage, leading to acute sleep deprivation and “Performance Drift.” This drift manifests as “No-Call, No-Shows,” leaving seniors in dangerous, unmonitored conditions for hours or days.
In contrast, a humanoid robot operates with Mechanical Invariance. It does not bring external stressors into the clinical environment. It has no personal financial crises, no marital stress, and no biological need for rest or recuperation. While a human caregiver’s patience and precision fluctuate based on their external life, a robot offers the same clinical vigilance during a difficult nocturnal episode as it does during a morning check-in. From an ethical standpoint, it is arguably more compassionate to provide a vulnerable patient with a predictable, high-performing machine than a volatile, exhausted human whose performance is compromised by the systemic pressures of low-wage labor.
VI. The RN Role: Systems Architect and Clinical Forensic Auditor
In this model, the Registered Nurse undergoes a professional evolution into two critical, multifaceted roles: the Clinical Systems Architect and the Clinical Forensic Auditor. These roles represent a departure from traditional bedside practice, necessitating a “pro vs. con” analysis of their operational and ethical impact on the nursing profession.
1. The Clinical Systems Architect: Designing the Algorithmic Standard
As a Systems Architect, the RN designs the “Clinical Red Lines”—the specific algorithmic thresholds for vitals, gait stability, and behavioral cues that trigger interventions.
2. The Clinical Forensic Auditor: Guarding the Chain of Custody
The Clinical Forensic Auditor manages the “Chain of Custody” for the patient’s physical and financial safety, reviewing robotic metadata to verify care integrity.
VII. Caregiver Synergy: The “Help, Not Replacement” Angle
It is essential to clarify that this model does not seek to eliminate the human caregiver; rather, it seeks to optimize them. High-performing Home Health Aides (HHAs) often welcome robotic partners because the robot assumes the “Heavy, Dirty, and Dangerous” tasks. These are the tasks—such as high-mass transfers that lead to musculoskeletal injuries and repetitive incontinent care that leads to burnout—that drive the industry’s 75% turnover rate.
By delegating the integrity-heavy and physically taxing labor to the robot, the human caregiver is freed to focus on what humans do best: empathy, companionship, and emotional support. The robot handles the “integrity tasks” (vitals, lifting, medication timing), while the human handles the “interpersonal tasks” (reminiscence therapy, social engagement). This synergy creates a sustainable workforce model where human caregivers are protected from injury and “compassion fatigue,” leading to higher job satisfaction and better patient outcomes.
VIII. Conclusion: Reliability as the Highest Form of Ethics
The home care industry is at a crossroads, facing a choice between maintaining a flawed status quo or embracing a more reliable future. We must move past the sentimental guilt associated with automation and ask the difficult ethical question: Is it negligent not to use a robot when we know the human-only model is prone to such high levels of undetected failure and volatility?
Protecting the most vulnerable members of our society requires systems that do not have “bad days,” do not suffer from “Performance Drift,” and cannot be compromised by financial desperation. By transforming the home from a “Domestic Black Box” into an auditable, data-driven environment, we empower Registered Nurses to act as the ultimate guarantors of safety. Reliability is not just a technical metric; it is the highest form of clinical ethics. The “Integrity Dividend” provided by humanoid robotics ensures that the sunset years of our population are defined by security, transparency, and the highest standard of professional care.
References
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026