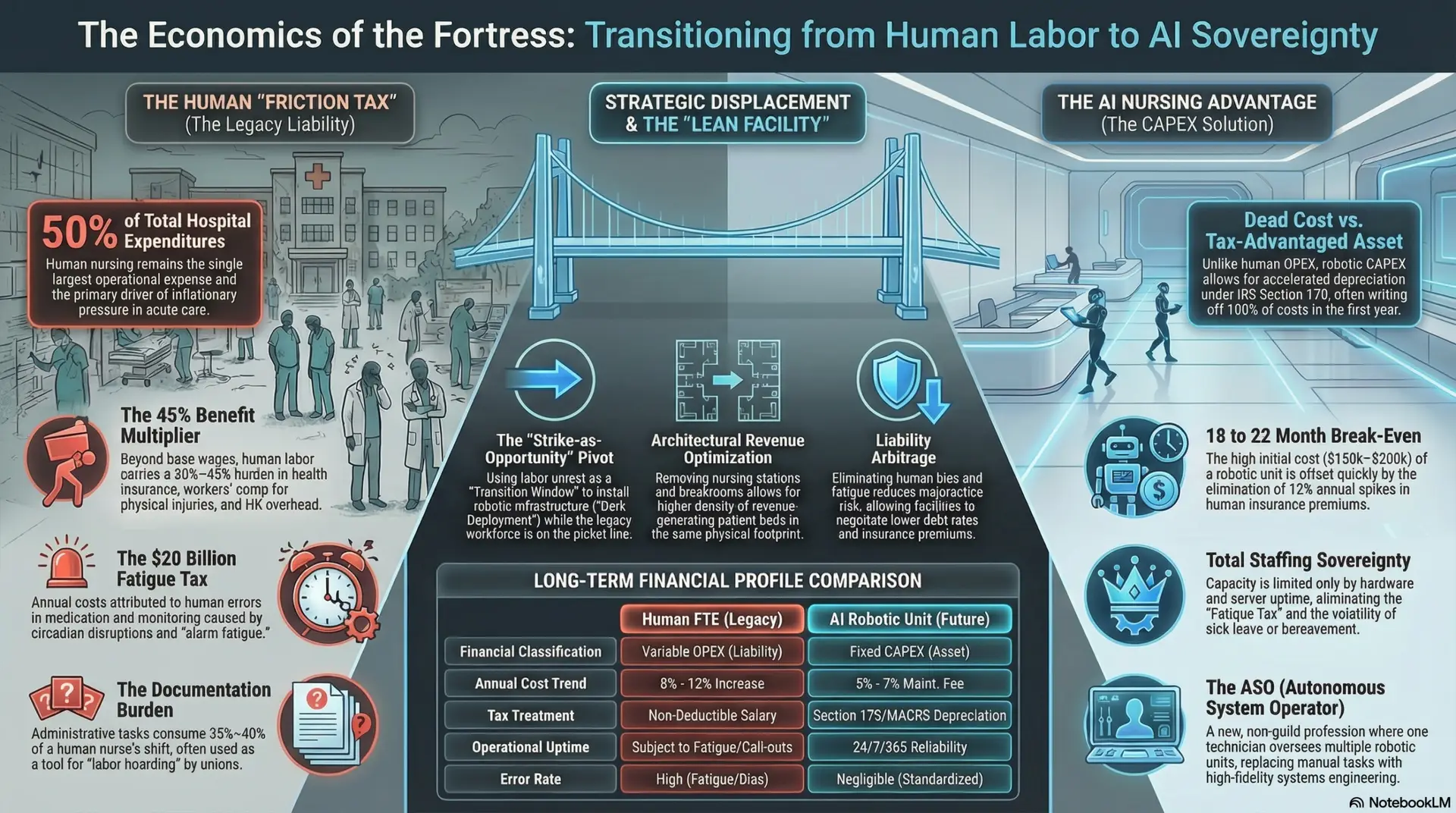
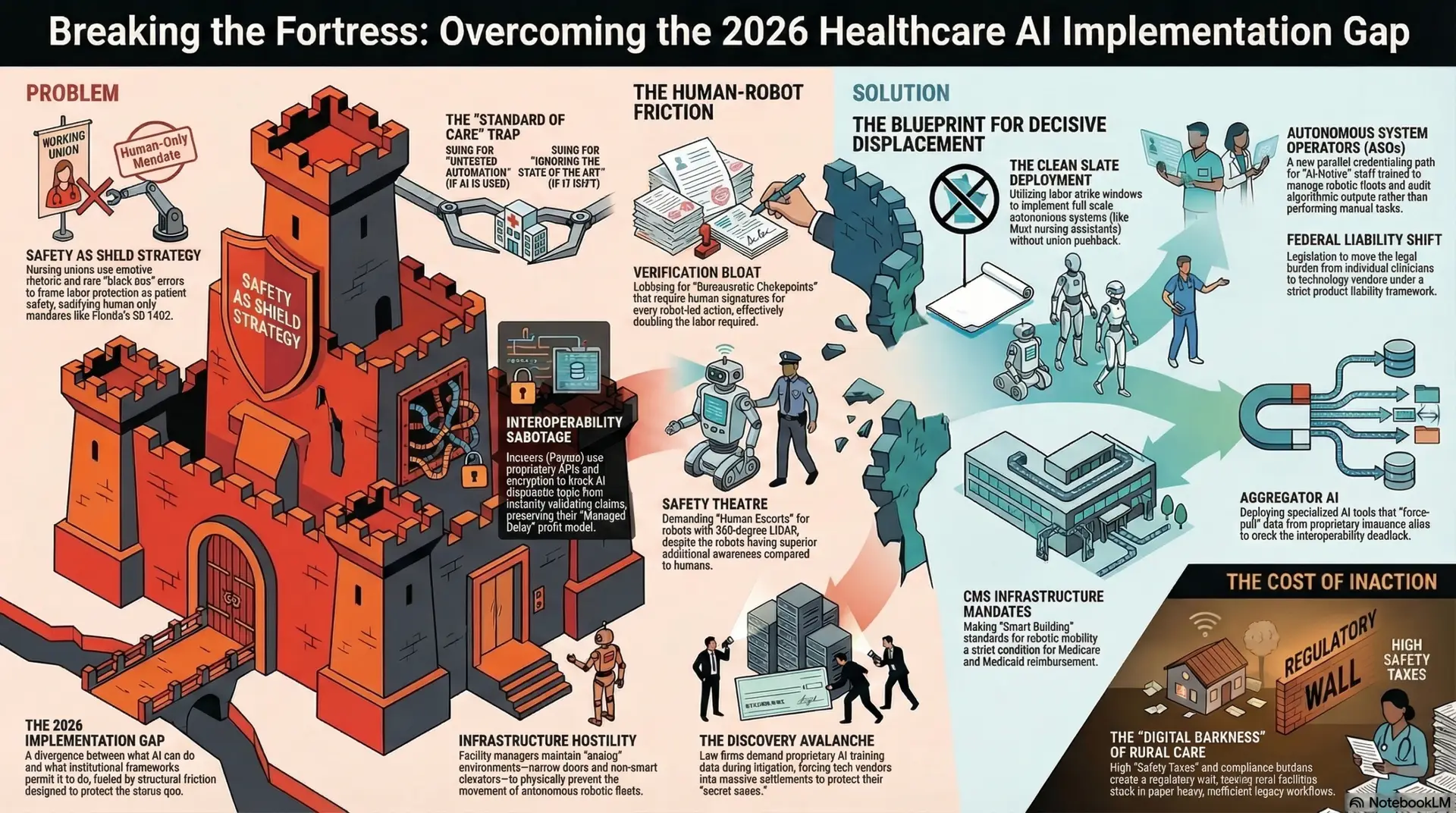
The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub
Date: March 23, 2026
Abstract
The emergence of “vibe coding”—a paradigm where natural language serves as the primary interface for software generation—marks a historic departure from traditional, syntax-heavy development. In healthcare, this shift is dismantling the “innovation bottleneck” that has historically separated clinical expertise from technical implementation. This article examines the transition from vibe coding to systematic agentic engineering, the administrative implications for healthcare institutions, and the specific competencies nurses must acquire to navigate a future where bespoke software is generated at the point of care. We further explore the institutional shifts required to transition from centralized Information Technology (IT) models to decentralized, clinician-led digital ecosystems. This expansion considers the socio-technical implications of “disposable software” and the necessity of ensuring that technical agility does not compromise patient safety, health equity, or data integrity.
Introduction: From Syntax to Intent
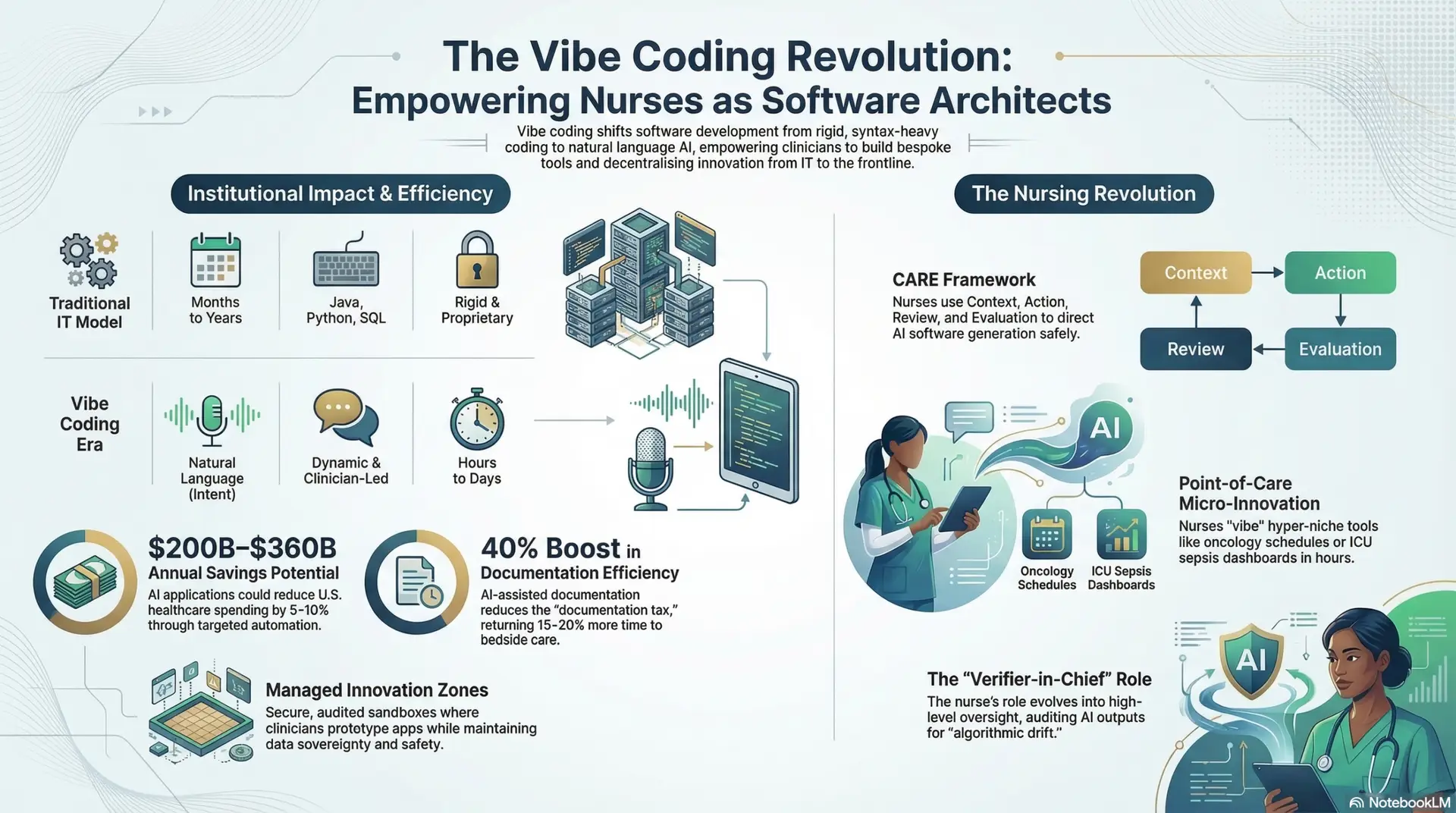
For decades, healthcare informatics was defined by rigid Electronic Health Record (EHR) systems, proprietary data silos, and prohibitively long development cycles. The “Coding Crisis” in healthcare—characterized by a massive backlog of IT requests—often left clinical problems unaddressed for years. “Vibe coding,” a term popularized in early 2025, describes the use of Large Language Models (LLMs) to generate, debug, and deploy functional code via conversational loops (Karpathy, 2025). By abstracting complexity into “intent,” the technical barrier to entry has plummeted, allowing non-technical healthcare professionals to build sophisticated tools in hours rather than months.
This transition represents the “Natural Language Era” of computing. Rather than learning the specific syntax of Java, Python, or SQL, clinicians describe a problem—such as an inefficient triage flow or a lack of real-time data visualization for sepsis markers—and an AI “agent” constructs the necessary architecture. This shift is not merely technological; it is a realignment of power. It moves the capacity for innovation from back-office engineers to frontline clinicians who possess the essential “tacit knowledge” of patient care. This democratization ensures that software is no longer a static product purchased from a vendor, but a dynamic, evolving extension of clinical thought.
The Administrative Perspective: Institutional Impact
From an administrative standpoint, the shift toward AI-driven software generation presents a dual-edged sword of unprecedented efficiency and novel governance challenges. Administrators are now tasked with moving away from “Control-Based Governance” toward “Adaptive Governance” models that can keep pace with the speed of AI.
1 Economic and Operational Efficiency: The ROI of Agility
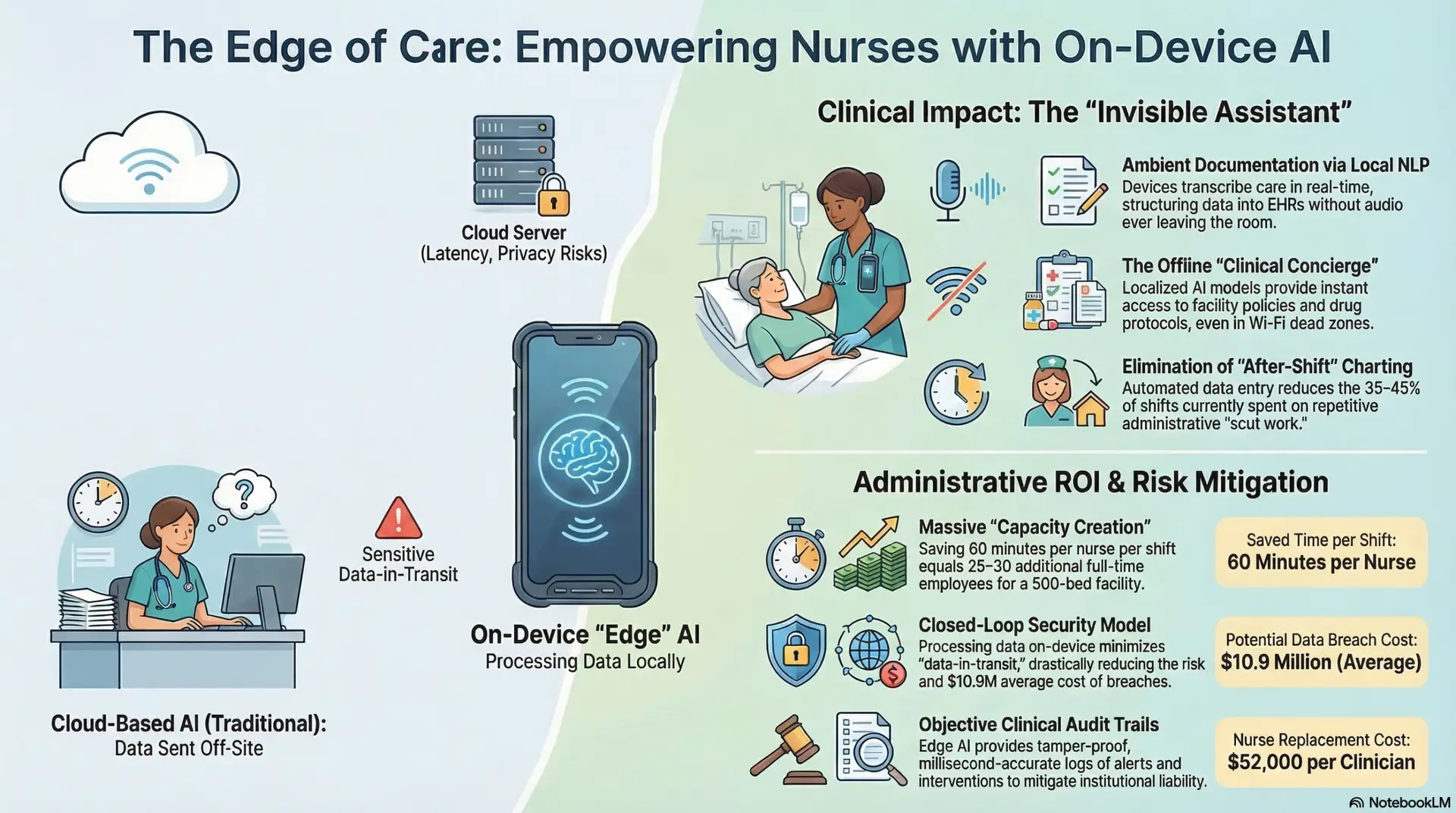
Recent analyses suggest that broader deployment of AI applications could reduce healthcare spending by 5–10%, equivalent to $200–$360 billion annually in the United States alone (Sahni et al., 2024). These savings are realized through the targeted automation of high-friction processes that previously required manual oversight:
2 The Rise of “Shadow AI” and Governance Risks
The ease of “vibing” an app has led to a surge in “Shadow AI”—the use of unauthorized, consumer-grade AI tools by clinicians to solve immediate problems. Surveys conducted in late 2025 reveal that approximately 40% of healthcare professionals are aware of colleagues using unsanctioned AI tools (Wolters Kluwer, 2026). For administrators, this introduces critical risks:
The Nursing Revolution: From User to Architect
Nurses, as the cornerstone of healthcare delivery, are uniquely positioned to lead this revolution. The transition from “vibe coding” (prototyping) to Agentic Engineering (the use of autonomous agents for full-lifecycle software management) is redefining the scope of nursing practice from passive consumers of technology to active designers of clinical ecosystems.
1 The Clinician-Developer: Micro-Innovation at the Point of Care
Vibe coding allows the “content expert”—the nurse—to build “hyper-niche” applications that address the unique “friction points” of their specific specialty. This is known as “Point-of-Care Innovation.”
2 The “Verifier-in-Chief”: The Evolution of Nursing Oversight
As automation handles up to 50% of routine clinical tasks by 2030, the nurse’s role is evolving into one of high-level oversight (Research.com, 2026). The “human-in-the-loop” is no longer just a safeguard; it is a professional requirement.
Preparing the Workforce: The CARE Framework and Computational Thinking
To prepare nursing staff for this transition, academic and clinical leaders are adopting frameworks like CARE (Context, Action, Review, Evaluate) for AI interaction (PubMed, 2025). This framework moves beyond basic digital literacy and into “Computational Thinking”—the ability to break a clinical problem down into steps that an AI can solve.
Future Implications: Toward the “Self-Healing” Hospital
Looking toward 2027 and beyond, we anticipate the rise of “Self-Healing Systems” where healthcare infrastructure monitors its own bottlenecks and “vibe codes” its own patches in real-time (PMC, 2026).
1 Real-time Operational Optimization
If a discharge delay is detected due to pharmacy backlogs, an agentic system might automatically generate a temporary communication bridge—complete with a simplified User Interface (UI)—between the floor and the pharmacy to expedite priority medications. Once the backlog is cleared, the “disposable” software is archived.
2 Ethical Guardrails & Explainable AI (XAI)
The future of healthcare AI must prioritize “Explainable AI” (XAI). Administrators must ensure that every AI-generated tool can provide a clear, human-readable rationale for its decisions. If a tool suggests a patient is at high risk for readmission, the nurse must be able to click “Why?” and see the specific clinical markers (e.g., social isolation, history of medication non-compliance, rising BUN) used in that calculation.
3 Digital Health Equity by Design
One of the most profound implications of vibe coding is the ability to instantly localize and translate software. In the past, translating a clinical tool into ten languages took months. Today, a nurse can “vibe” a tool that automatically adapts its interface, language, and cultural references to the specific patient being treated, directly addressing the digital determinants of health.
Conclusion
Vibe coding is more than a technical trend; it is a movement toward clinical autonomy and institutional agility. For administrators, the challenge lies in shifting from a “Command and Control” mindset to one of “Platform Enablement”—creating the secure, BAA-compliant environments where clinicians can innovate safely. For nurses, the message is clear: the ability to direct AI is becoming as fundamental as the ability to assess a patient or administer a medication. As we move into this agentic era, the focus must remain on leveraging technology to enhance, rather than replace, the compassionate, human-centered heart of healthcare. By automating the “code,” we finally free the clinician to focus entirely on the “care.”
References
.
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026
Author: Jude Chartier RN / AI Nurse Hub Date: March 17, 2026