The Vibe Coding Revolution: Democratizing Healthcare Software Development and the Future of Nursing Practice
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
Author: Jude Chartier RN / AI Nurse Hub
Date: March 30, 2026
Abstract
The global healthcare sector is currently embroiled in an unprecedented fiscal crisis, exacerbated by a structural reliance on escalating labor costs and systemic inefficiencies inherent in legacy, human-centric care models. This report, commissioned by AI Nurse Hub, provides an exhaustive examination of the economic viability of “Decisive Displacement”—the strategic and wholesale replacement of legacy nursing labor with autonomous, embodied artificial intelligence (AI). By rigorously quantifying the “Friction Tax” associated with human nursing—including the hidden costs of biological fatigue, guild-based scarcity, and administrative sabotage—this analysis demonstrates a clear, data-driven path toward institutional solvency.
Furthermore, it reframes labor unrest not as a disruption to be mitigated through concession, but as a strategic “Transition Window” for capital expenditure (CAPEX) deployment. Key findings suggest that while the transition faces fierce institutional resistance from entrenched guilds, the long-term benefits of robotic reliability, tax-advantaged depreciation under IRS guidelines, and standardized care protocols render the displacement of the traditional nursing guild an economic and clinical inevitability. The report concludes that institutional survival in the late 2020s depends entirely on the resolve of administrators to dismantle the “Fortress of Resistance” through aggressive technological capitalization, ultimately shifting the healthcare paradigm from a variable-cost human service to a fixed-cost technological utility.
Introduction
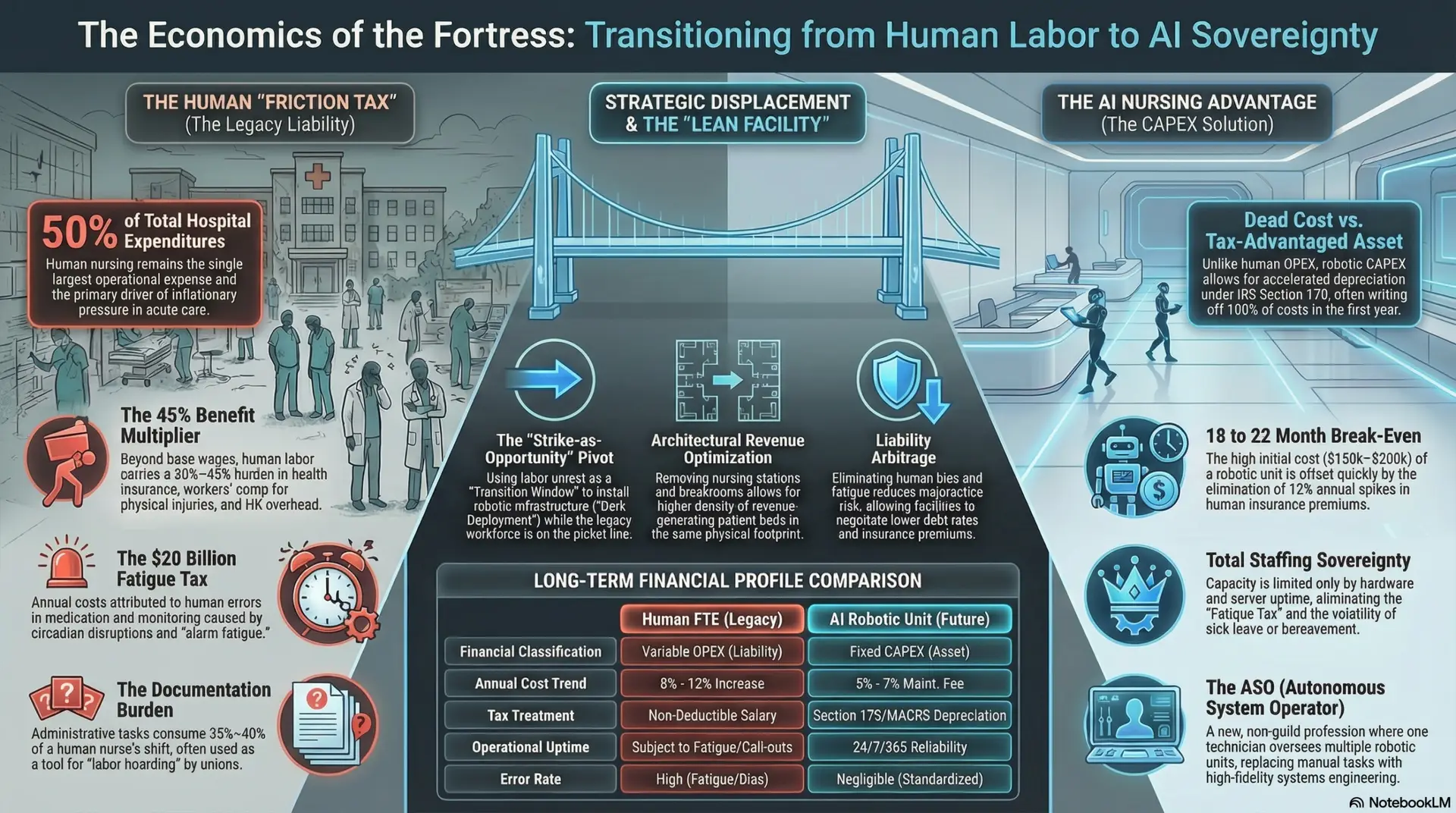
As of early 2026, the modern healthcare landscape has reached a fiscal breaking point, characterized by an unsustainable reliance on high-cost, high-variability human labor. Nursing labor remains the single largest operational expense (OPEX) for acute care facilities, often accounting for over 50% of total hospital expenditures and serving as the primary driver of inflationary pressure within the sector. Despite massive investment in “human-centric” retention programs, wellness initiatives, and sign-on bonuses, the industry remains plagued by chronic burnout, volatility, and the inherent biological limitations of the human clinician. This report, true to the mission of AI Nurse Hub, moves past the sentimentalism often found in healthcare discourse to delve into an uncomfortable fiscal reality: the “Fortress of Resistance” built by nursing unions and legacy institutional frameworks is now the primary barrier to a more efficient, safer, and financially stable healthcare system.
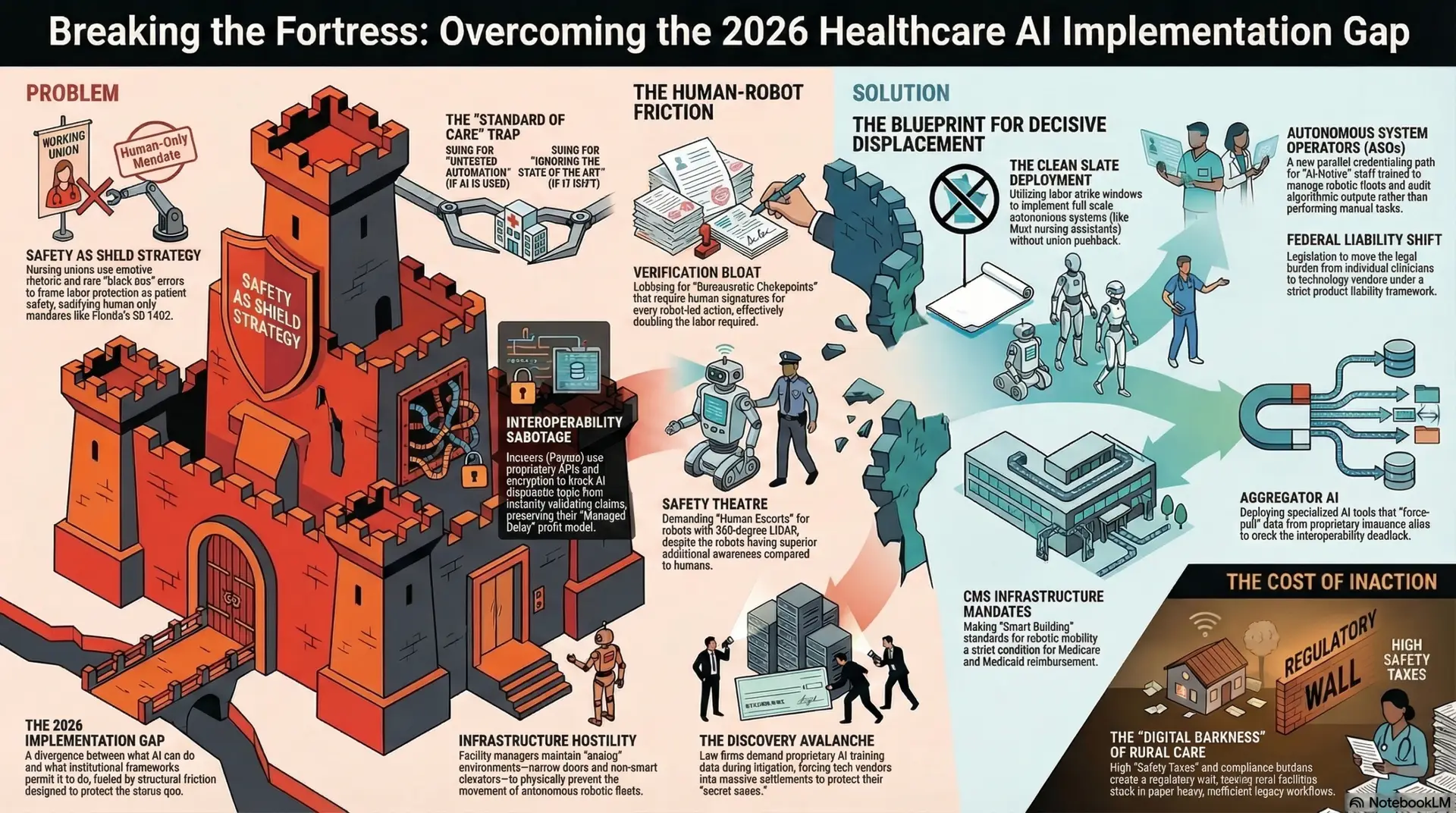
The “Implementation Gap” of 2026 is no longer a technological hurdle but a political and institutional one. We possess the algorithmic precision to diagnose and the robotic dexterity to deliver care, yet we remain shackled to a 19th-century guild model that prioritizes labor protectionism over patient throughput and fiscal health. While many contemporary analyses focus on the emotional or social “value” of nursing, this analysis outlines a hardline economic transition to fully automated nursing protocols. It prioritizes institutional survival and clinical precision over legacy labor paradigms, arguing that the traditional “guild model” of nursing is a relic of an analog era that cannot survive the transparency, speed, and 24/7 reliability of an AI-ubiquitous market. To ensure fiscal sovereignty and protect shareholder value, healthcare leadership must move beyond incremental pilots and embrace a strategy of decisive, total displacement.
The Nursing “Friction Tax” (Labor Audit)
The current human-labor model imposes a significant, though frequently obfuscated, “Friction Tax” on healthcare systems. This tax is a composite of direct compensation, indirect liabilities, and the massive hidden costs associated with human error and cognitive variability. To understand the economic necessity of displacement, one must first audit the true cost of a human “FTE” (Full-Time Equivalent) in the high-acuity environment, accounting for factors typically omitted from standard payroll projections.
Direct Nursing Labor Costs and the FTE Burden
The FTE burden for a staff nurse extends far beyond the base hourly wage, creating a complex web of financial commitments that drain hospital liquidity and stifle innovation. According to the Bureau of Labor Statistics (2025), the “Benefit Multiplier” for licensed healthcare professionals has risen to between 30% and 45%. This multiplier encompasses not only health insurance and employer-paid payroll taxes but also workers’ compensation premiums—which are significantly higher for human staff prone to back injuries and repetitive stress—paid leave, and the massive overhead of human resources management required to arbitrate interpersonal disputes and compliance issues.
When adjusted for the rising costs of these non-wage benefits, a human nurse represents a variable cost that escalates annually at a rate far exceeding the Consumer Price Index (CPI). Unlike fixed technological assets, which remain predictable over their five-to-ten-year lifecycle, human labor costs are subject to the whims of collective bargaining and market-driven “bidding wars” for travel nurses, which can triple labor costs in a single quarter during local shortages. Furthermore, the “Guild Pension Liability”—the accumulation of long-term, defined-benefit retirement commitments—creates a massive, non-liquid drag on hospital balance sheets. These liabilities often negatively impact hospital bond ratings, increasing the cost of borrowing for critical infrastructure projects. In essence, the human nurse is an appreciating liability that consumes capital, whereas the AI nurse is a depreciating, tax-advantaged asset that produces it.
The Fatigue Tax and Synergistic Biological Failures
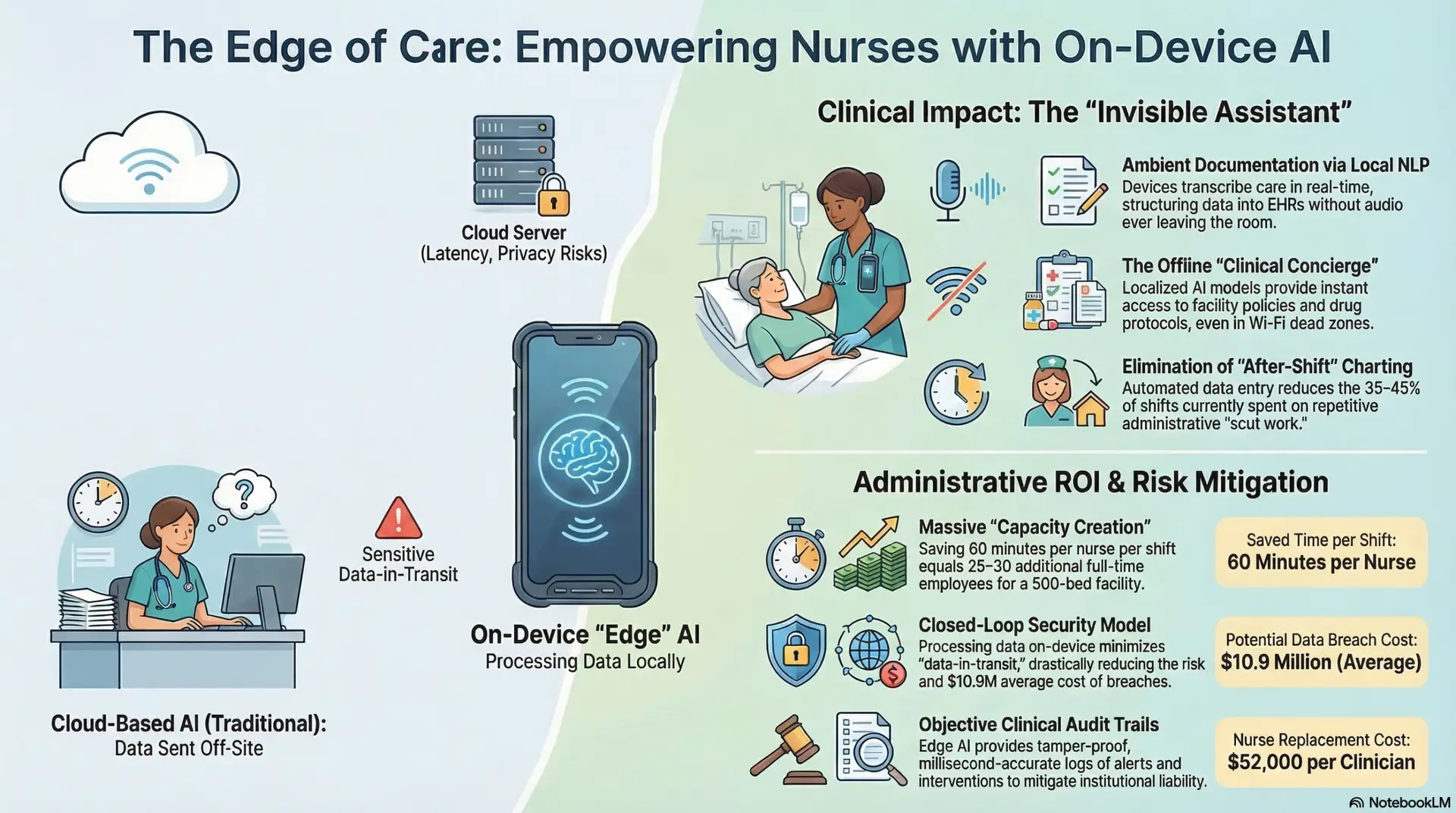
Beyond direct compensation, human biology introduces a “Fatigue Tax” into clinical workflows that no amount of “resilience training” or “wellness retreats” can fully mitigate. The Institute of Medicine (2024) estimates that human error in medication administration and patient monitoring—often attributed to shift-fatigue, circadian rhythm disruptions, and cognitive “alarm fatigue”—costs the U.S. healthcare system approximately $20 billion annually. Human clinicians represent a liability that automated protocols effectively neutralize.
The biological “signal-to-noise” ratio in human practitioners is inherently flawed. For instance, an embodied AI system does not experience “decision fatigue” at the tenth hour of a shift, nor does it suffer from “recency bias” or “omission bias” that can lead to catastrophic diagnostic errors. Algorithms do not have “bad days,” they do not experience interpersonal conflict with colleagues that distracts from patient care, and they do not require emotional regulation pauses. By implementing AI-driven diagnostic and documentation protocols, the administrative drag on the remaining frontline architecture is significantly lessened. This synergy allows for a more streamlined, “top-of-license” operational structure where clinical decisions are dictated by high-fidelity, real-time data rather than subjective, often idiosyncratic human intuition which varies wildly across shift changes and individual moods (Zhang et al., 2026).
The “Strike-as-Opportunity” Strategy
Labor unrest, traditionally viewed by hospital boards as a catastrophic disruption to be settled at any cost, must be strategically reframed as a “Transition Window” for structural displacement. The nursing strike is the ultimate manifestation of the “Fortress of Resistance,” but it is also the fortress’s greatest vulnerability—a moment where the “human-in-the-loop” is voluntarily removed, providing an opening for permanent automation.
The Crisis-to-CAPEX Pivot and “Dark Deployment”
Nursing strikes currently impose an average cost of $2 million to $3 million per day on large facilities due to the exorbitant rates of travel nurses, legal counsel fees, security overhead, and lost surgical revenue (American Hospital Association, 2025). Rather than viewing these funds as a total loss or “the cost of doing business,” forward-thinking administrations can pivot this capital toward the procurement of robotic vitals-capture fleets and autonomous transporters.
This “Dark Deployment” strategy involves the tactical installation of the physical and digital infrastructure for automation while the legacy workforce is on the picket line. By utilizing the physical absence of the unionized workforce, hospitals can bypass the internal sabotage, “slow-walking,” and “safety-concern” theater that typically occurs during collaborative transitions. When the strike concludes, the hospital does not return to the previous status quo; it returns with 30% to 50% of its manual tasks already automated, allowing for permanent headcount reductions and a refusal to re-hire non-essential striking staff. The strike, intended to exert leverage, instead facilitates the permanent removal of that leverage through the rapid instantiation of capital assets.
Staffing Consistency vs. Biological Scarcity
Staffing a 24/7 facility with human labor requires managing a volatile web of “call-outs,” sick leave, bereavement, and turnover. Each “hole” in the schedule creates a cascading economic effect, often requiring mandatory overtime at 1.5x or 2x pay rates, which further exacerbates the “Fatigue Tax” and fuels the burnout cycle. Robots, however, eliminate labor scarcity entirely.
An automated workforce ensures 100% adherence to clinical protocols without the “shortcut” behaviors or “informal workarounds” common in high-stress human shifts. This provides a level of operational reliability and predictability that human guilds, governed by biological needs and collective bargaining agreements, simply cannot match. The facility gains “Total Staffing Sovereignty,” where care capacity is limited only by hardware availability and server uptime, not by the availability or temperament of a volatile human labor market. This shift allows for “Level Loading” of hospital operations, where the cost of a Tuesday afternoon is identical to that of a Saturday night.
The Robotic CAPEX vs. Human OPEX Deep Dive
The core of the economic argument for displacement lies in the fundamentally different financial treatments of capital assets versus operational labor. This is the “hidden lever” that makes the transition not just possible, but fiscally superior for long-term growth and investor confidence.
Financial Treatment, Tax Advantages, and Section 179
Human nursing labor is a recurring Operational Expense (OPEX) with no residual value; it is a “dead” cost that must be paid in perpetuity with no equity gain. In contrast, robotic units are Capital Expenses (CAPEX). Under Internal Revenue Service (2025) guidelines, specifically Section 179 and the Modified Accelerated Cost Recovery System (MACRS), hospitals can utilize accelerated depreciation to write off the majority of robotic procurement costs—often 100% up to certain limits—in the first fiscal year.
This provides massive end-of-year tax relief, effectively subsidizing the transition to automation in a way that is legally impossible with human salary expenditures. For a profitable health system, the tax savings alone can cover a significant portion of the initial robotic fleet cost. Furthermore, capital assets can be used as collateral for further financing, whereas a human workforce is a persistent liability that decreases creditworthiness and increases the cost of capital. Moving from OPEX to CAPEX turns “labor” into a balance sheet strength rather than an income statement weakness.
Total Cost of Ownership (TCO) and the “Break-Even” Realities
While a high-performance robotic nursing unit may have an initial procurement cost of $150,000 to $200,000, its TCO over a five-year period is significantly lower than that of a total-compensation human nurse. The National Bureau of Economic Research (2026) projects a financial “Break-Even Point” of approximately 18 to 22 months. Beyond this point, the 5% to 7% annual maintenance and software fees are negligible compared to the 8% to 12% annual increase in human health insurance premiums and the inevitable “step increases” in salary demanded by labor unions.
Transitioning to a CAPEX-heavy model allows the hospital to treat its “staffing” as an amortizable asset that improves the balance sheet and enhances EBITDA. Additionally, the marginal cost of adding a bed in an automated facility is a fraction of that in a traditional one. In the autonomous model, increasing capacity requires only a marginal increase in SaaS licensing and electricity; in the legacy model, it requires hiring a new human FTE with all the associated “Friction Tax” burdens and the space-inefficient infrastructure (breakrooms, nursing stations) required to support them.
Neutralizing Administrative Sabotage
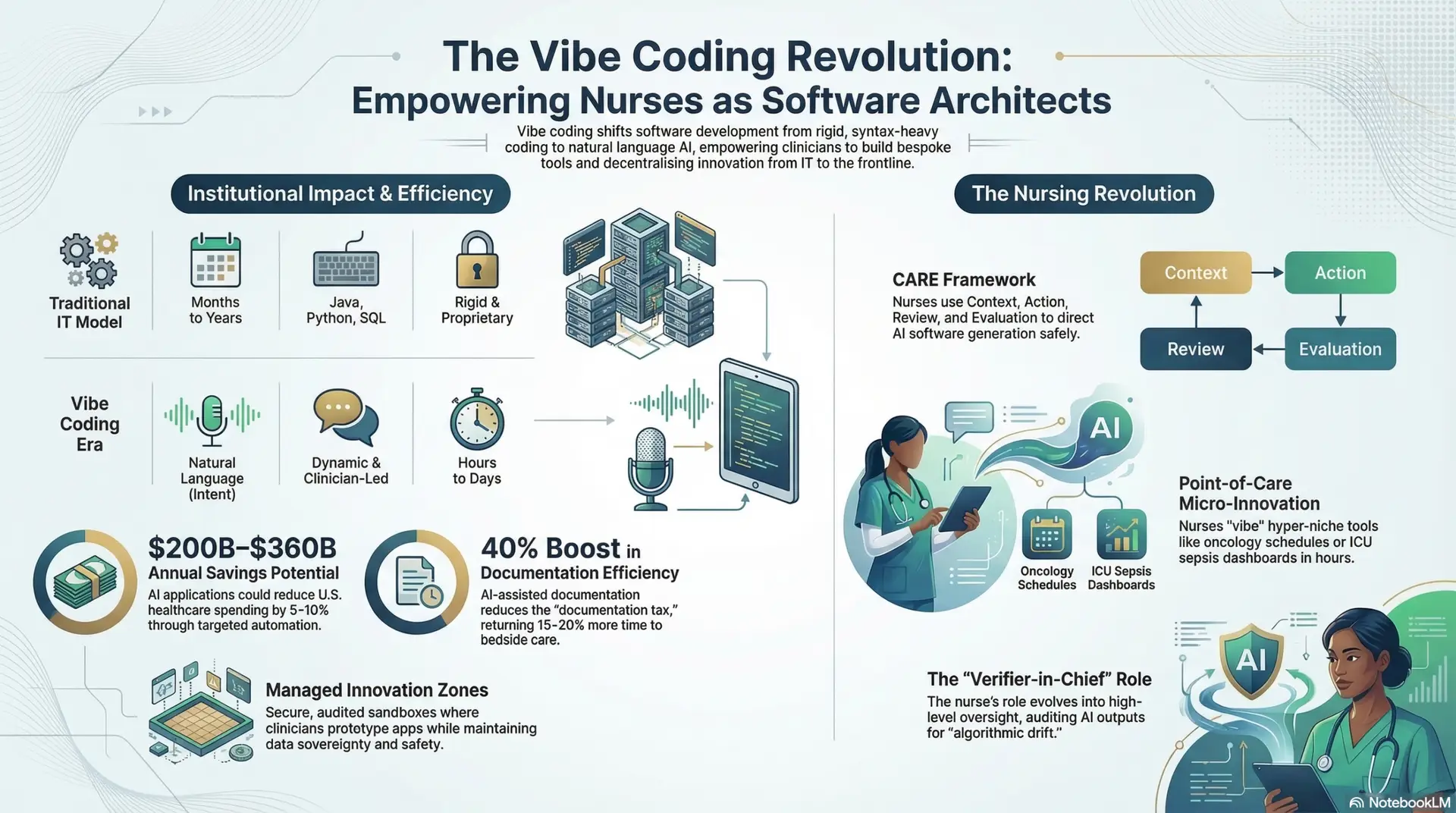
The transition to autonomous nursing is further supported by the automation of the “Documentation Burden,” which currently consumes approximately 35% to 40% of a staff nurse’s shift (Hing et al., 2024). This burden is often used as a tool for administrative sabotage by unions, who argue that high documentation requirements necessitate even higher staffing ratios, creating a circular logic of labor expansion known as “labor hoarding.”
By utilizing AI-led charting, ambient voice recognition, and real-time audit-readiness protocols, facilities can eliminate the need for human medical record auditors and reduce the legal risks associated with incomplete, “noised,” or retaliatory data entry. Automation transforms documentation from a labor-intensive chore into a passive, background data-stream. This removes the union’s primary argument for “staffing-grid” increases, further justifying a leaner human workforce and exposing the “Documentation Crisis” as a manufactured friction designed to protect and expand labor slots at the expense of hospital solvency. In an automated system, “charting” becomes a byproduct of care rather than a justification for labor.
The Nursing “Premium Pivot” and Market Disruption
Facilities that successfully break the “Fortress of Resistance” through automation gain an insurmountable competitive advantage in the 2026 healthcare marketplace, essentially becoming “Category Killers” within their regional markets.
Volume Optimization and the “Lean Facility” Model
Automation allows for significantly higher patient throughput without a corresponding increase in labor costs. The “Lean Facility” operates with a radically reduced overhead, allowing it to achieve profitability at lower reimbursement rates than its competitors. While the primary focus of this report is nursing, the ancillary benefits of automated logistics, janitorial robotics, and pharmacy automation create an ecosystem where every square foot of the facility is optimized for patient care rather than staff accommodation.
For instance, the removal of large nursing stations, staff locker rooms, and breakrooms allows for a higher density of revenue-generating patient beds within the same physical footprint. This architectural efficiency increases the revenue-per-square-foot metric, a key indicator of institutional health. The “Lean Facility” model also allows for more flexible scheduling of procedures, as the robotic workforce does not require the traditional “shift change” lulls that currently slow down hospital throughput in the early morning and late evening.
The Safety Premium and Liability Arbitrage
Robotic precision fundamentally alters the risk profile of the acute care environment. Lower malpractice risk—driven by the elimination of fatigue-related errors, distraction-based oversights, and medication “near-misses”—allows facilities to negotiate more favorable institutional debt rates and significantly lower insurance premiums. Standardized, error-free care becomes a marketable “Safety Premium” that attracts both discerning patients and institutional investors.
In an era of mandatory price transparency, the facility that has displaced its high-cost, high-variability labor with low-cost, high-reliability AI will inevitably capture the majority of the market share. Legacy “guild-based” hospitals will be left with a higher-risk, higher-cost patient pool and will eventually collapse under the weight of their own uncompetitive labor structures and skyrocketing malpractice rates. This creates a “Liability Arbitrage” opportunity where the automated facility wins by simply being less human—and thus less risky.
Overcoming Resistance and Narrative Control
The resistance to full automation will be fierce, rooted in deep-seated fears of professional obsolescence and the carefully curated mythos of the “human touch.” However, this resistance can be overcome through meticulous planning and a powerful narrative pivot that prioritizes patient survival and clinical purity over employment statistics.
The “Humanity Through Automation” Narrative
The narrative must move past the “Job Loss” frame and focus exclusively on “Error-Free Care.” By highlighting how automation saves lives by eliminating the fatal consequences of human fatigue, distraction, and inherent bias, the public focus shifts from the plight of the displaced worker to the safety of the patient. Resistance to automation is thus reframed as resistance to patient safety.
The marketing strategy should emphasize that machines are “purer” than humans—they do not bring their personal problems to the bedside, they do not have prejudices, and they never forget a detail. The “human touch” is rebranded as “human risk.” In this new narrative, the most “human” thing a hospital can do is remove the fallible human from the critical path of care. Public relations campaigns should feature data-driven comparisons showing the reduction in hospital-acquired infections and medication errors in automated wards versus traditional ones.
“Human-in-the-Loop” Supervisory Hubs and ASO Credentials
To satisfy skeptical regulators and provide a “social safety net” for the transition, the model includes the deployment of remote “Human-in-the-Loop” supervisory hubs. These hubs allow for a single “AI-Native” technician—certified as an Autonomous System Operator (ASO)—to oversee multiple robotic units across several wards. This maintains a human presence in the oversight process while removing the human from the high-error, high-cost physical tasks.
These ASOs represent a new, non-guild-based profession that is easier to train and more scalable than traditional nursing. The curriculum for ASOs focuses on systems engineering, ethical oversight, and “human-exception” management rather than manual tasks like vitals-taking or wound cleaning. AI Nurse Hub acknowledges that “Decisive Displacement” is a deeply unpopular topic among legacy practitioners; however, professional persistence requires delving into these uncomfortable truths. To ignore the economic inevitability of automation is to invite the total fiscal collapse of the healthcare system. The fiscal survival of the ecosystem depends on the resolve of administrators to move past legacy guild models.
Conclusion: The Economic Inevitability
The data suggests that by 2030, the cost of maintaining the legacy human nursing “Fortress” will exceed the total solvency of the modern health system. The Net Displacement Value (NDV) of moving to an automated, CAPEX-based model is overwhelmingly positive, offering a reduction in OPEX that can be reinvested into advanced medical technology, facility expansion, and shareholder returns.
To ensure long-term institutional viability, immediate strategic pivots toward robotic nursing are not merely an option—they are a clinical and fiscal imperative. The healthcare leaders who choose to break the friction today, leveraging labor strikes and tax-advantaged capital to reset their workforce, will be the only ones left standing in the automated landscape of tomorrow. The “Fortress” is crumbling; its walls of protectionist guilds and administrative friction are no longer enough to withstand the economic reality of AI. The only question remains whether administrators will be crushed by its fall or choose to build a more efficient, autonomous architecture in its place.
References
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026
Author: Jude Chartier RN / AI Nurse Hub Date: March 17, 2026