The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub
Date: March 4, 2026
Abstract
The American home care industry is currently navigating a dual crisis defined by a massive labor shortage and systemic safety failures. As the caregiver-to-patient ratio continues to widen, the emergence of embodied humanoid robotics offers a transformative solution to these challenges. This article proposes a comprehensive scholarly framework for a nurse-led hybrid model, where the Registered Nurse (RN) serves as a Clinical Systems Architect. By integrating technical algorithmic logic with the legal architecture of digital delegation, this model redefines clinical governance. Drawing upon Peplau’s Theory of Interpersonal Relations and Locsin’s Theory of Technological Competency as Caring, the paper argues that humanoid robots function as mechanical surrogates. This surrogacy allows nurses to transcend the physical exhaustion of repetitive labor and focus on high-acuity clinical judgment, complex triage, and therapeutic intervention. This framework positions the RN at the center of a technologically augmented care ecosystem, ensuring that automation serves to enhance, rather than replace, the human element of nursing, while simultaneously stabilizing the economic volatility of the home care sector.
Introduction
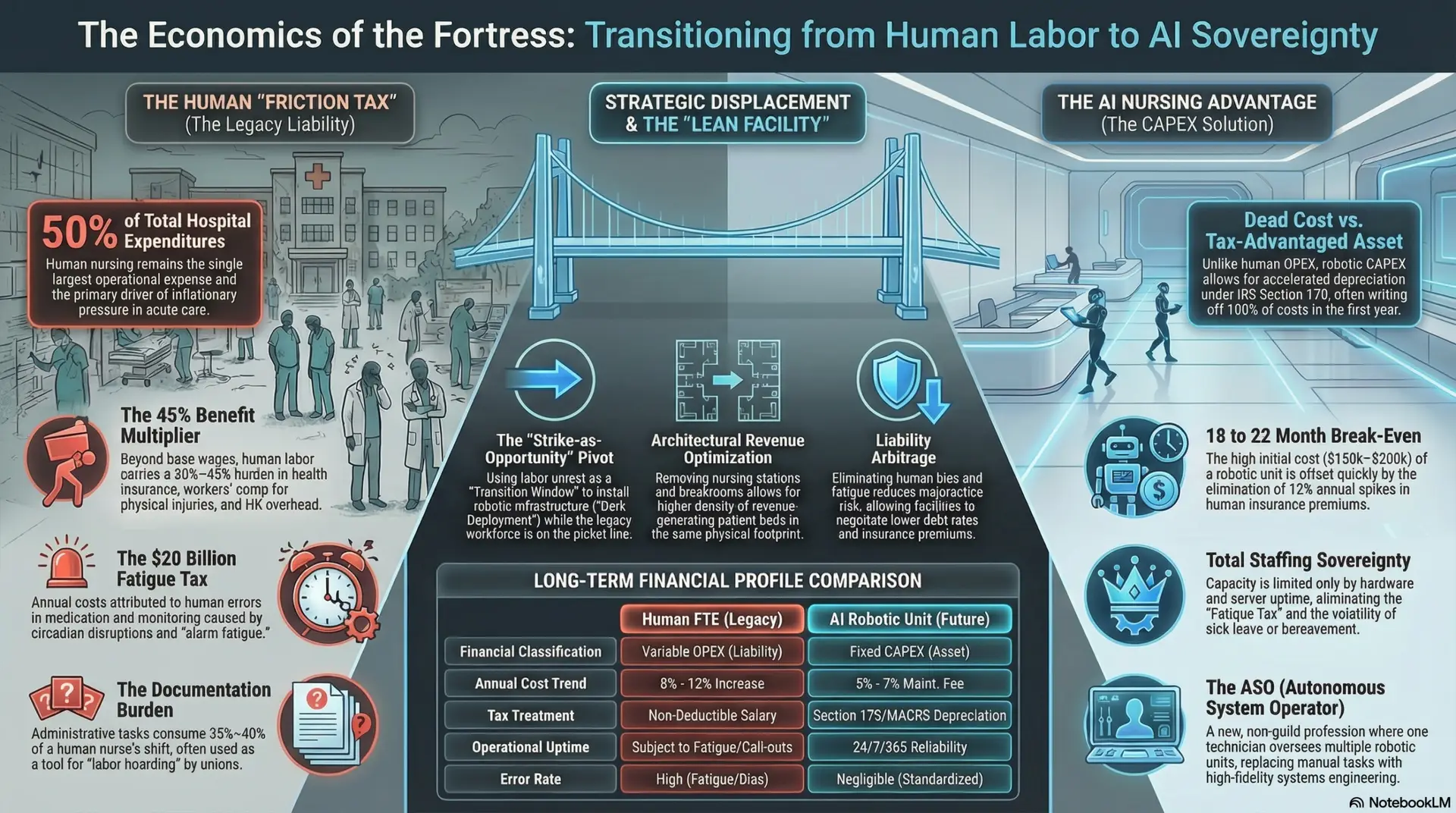
As the global population ages, the demand for home-based geriatric care has reached a critical inflection point. By 2030, one in five Americans will be over the age of 65, creating a demographic shift often referred to as the “silver tsunami.” Traditional healthcare infrastructures, designed for acute, episodic intervention, are fundamentally ill-equipped for the sustained, high-fidelity monitoring required by this population. Current models, heavily reliant on human-capital-intensive labor, are increasingly characterized by staggering turnover rates—ranging from 75% to 100% annually—and significant biological variability in care quality (Activated Insights, 2025).
Human caregivers, particularly home health aides (HHAs), are among the lowest-paid workers in the economy, often subjected to grueling schedules and high-stress environments. This leads to a systemic cycle of “Compassion Fatigue,” where emotional exhaustion results in neglect, irritability, or an inability to identify subtle clinical changes. Furthermore, human labor is subject to “Biological Variability”—fluctuations in performance dictated by mood, sleep deprivation, or personal distraction. These variables cumulatively degrade patient safety and increase agency liability.
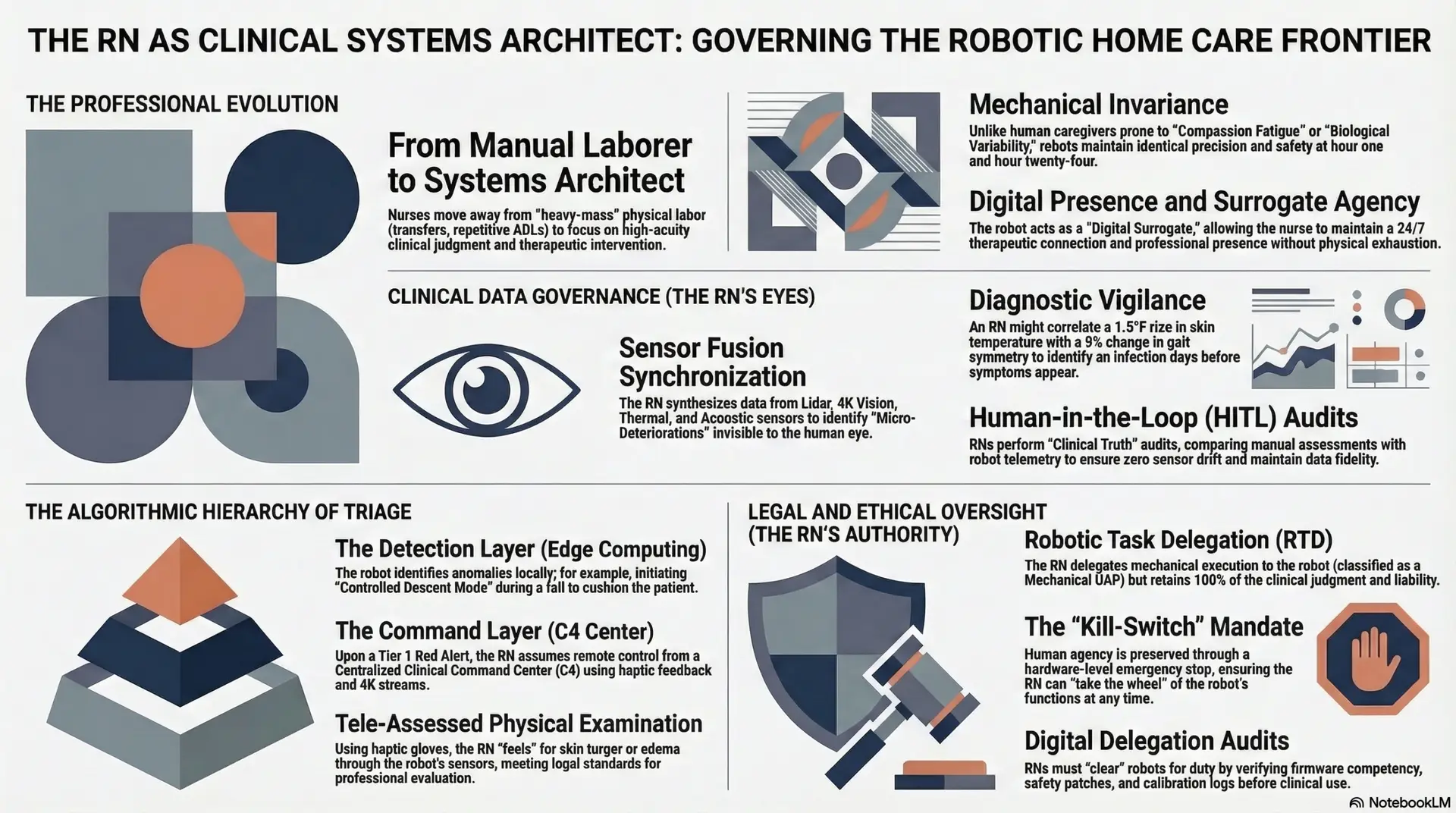
The introduction of humanoid robotics into the domestic environment represents a paradigm shift from reactive, incident-based care to predictive, continuous monitoring. This transition, however, is not merely a mechanical upgrade; it is a professional evolution. To be clinically sound and ethically viable, these systems must be governed by Registered Nurses (RNs). As the only professionals equipped with both deep clinical expertise and the legal license to exercise complex judgment, RNs must manage the high-frequency data streams and ethical complexities inherent in these autonomous systems. This paper explores how the RN evolves into a “Systems Architect,” leveraging “Mechanical Invariance”—the ability of a machine to perform a task with identical precision at hour one and hour twenty-four—to stabilize an industry currently defined by human exhaustion and volatility.
Theoretical Framework: Peplau’s Interpersonal Relations in the Digital Age
Hildegard Peplau’s Theory of Interpersonal Relations (1952) remains a cornerstone of nursing practice, defining nursing as a significant, therapeutic, and interpersonal process. Critics of automation often argue that robotics may diminish the “human element,” yet a re-examination of Peplau’s four phases—Orientation, Identification, Exploitation, and Resolution—suggests that humanoid surrogacy can actually strengthen the nurse-patient bond by removing the friction of task-saturated, “heavy-mass” labor.
When a nurse is no longer physically exhausted by the mechanical requirements of home care, they can devote cognitive and emotional energy to the patient’s psychological landscape. The robot acts as a “Digital Surrogate,” providing a continuous presence that allows the nurse to maintain a therapeutic connection across time and space. This aligns with Rozzano Locsin’s (2005) theory of Technological Competency as Caring, where the nurse’s expertise is expressed through the precise configuration and oversight of the technology. The robot does not replace the nurse; it extends the nurse’s presence, ensuring that the patient feels monitored, supported, and safe 24/7.
Clinical Data Governance and the Bio-Digital Feedback Loop
The RN’s role in this new paradigm is defined by Clinical Data Governance. Humanoid robots, equipped with a sophisticated sensor fusion suite (Lidar, 4K Computer Vision, Thermal imaging, and Acoustic sensors), generate gigabytes of daily health data. This creates what is termed the Continuous Bio-Digital Feedback Loop, where every movement, physiological shift, and behavioral pattern is recorded and analyzed.
Technical Workflow: The Algorithmic Hierarchy of Triage
To manage the immense labor of constant monitoring, the RN utilizes a nested logic gate system. This technical workflow ensures that life-threatening “signals” are escalated instantly while “noise” is filtered at the “edge” (the robot’s onboard computer).
The Licensure Framework: Digital Delegation and Surrogate Liability
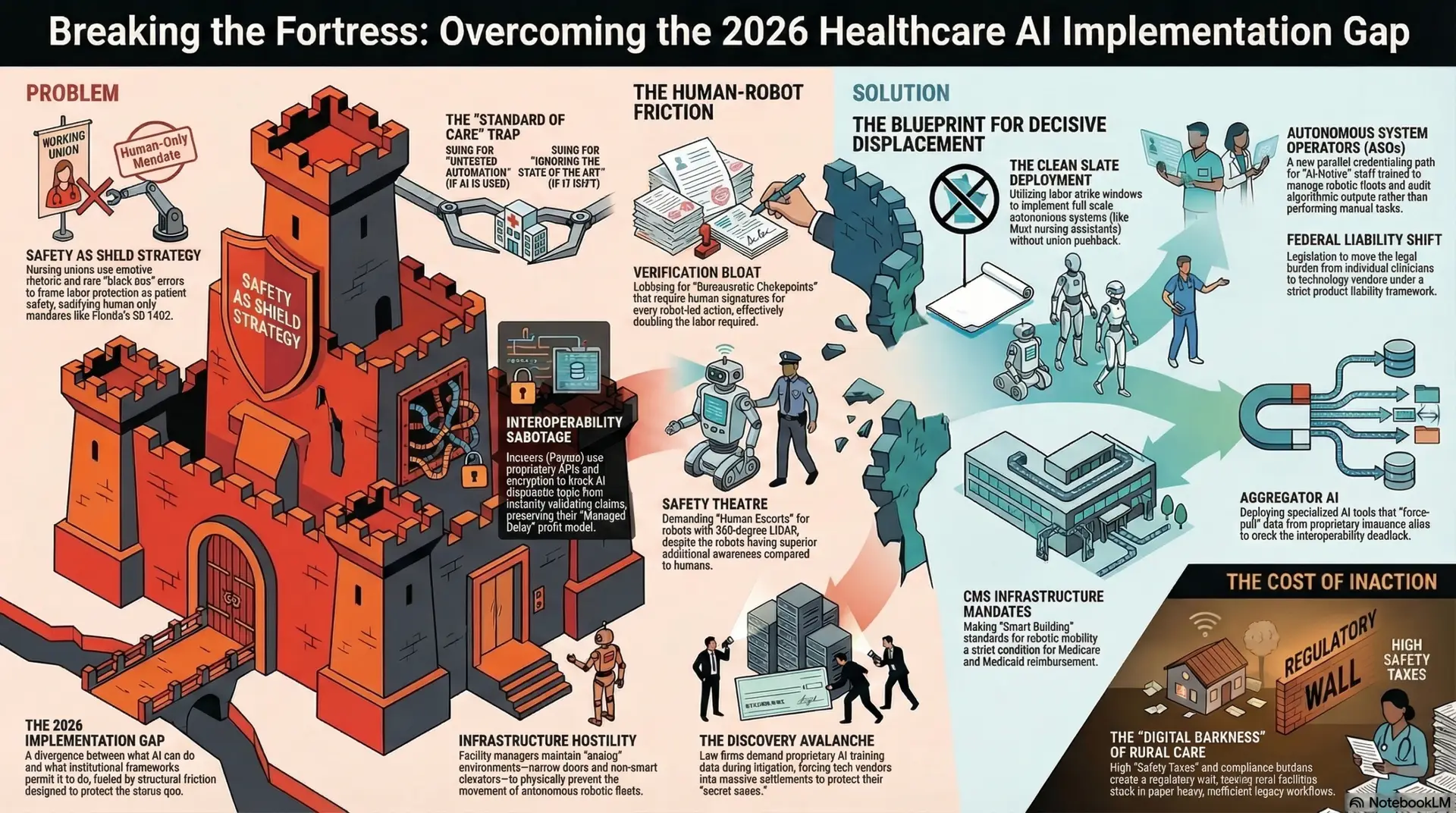
A primary barrier to widespread robotic adoption is the question of legal authority. This framework proposes a radical shift in nursing law by officially classifying the humanoid robot as a Mechanical Unlicensed Assistive Personnel (UAP).
Under the Robotic Task Delegation (RTD) Standard, the RN delegates the mechanical execution of a task but never the clinical judgment. This creates a state of Surrogate Liability, where the RN’s license “covers” the robot’s actions. Just as an RN is responsible for the tasks delegated to a human aide, the RN is responsible for the “Firmware Competency” of the robot.
The Surrogate Practice Act advocates for three core pillars:
Case Study: Management of a Traumatic Mechanical Fall
Consider the case of an 82-year-old female patient with advanced osteoporosis living alone. During a robotic-assisted transfer from bed to a wheelchair at 02:00, a sudden mass shift occurs due to patient orthostatic hypotension. The robot’s torque sensors detect the imbalance within milliseconds and execute a “Controlled Descent,” positioning its padded torso to cushion the patient’s head and hip.
Instantly, the RN in a Centralized Clinical Command Center (C4) receives a Tier 1 Red Alert on a haptic wearable. Within seconds, the RN is viewing the live 4K feed via the robot’s head-mounted cameras. Utilizing macro-zoom capabilities, the RN identifies immediate clinical indicators of a fractured hip: the right leg is externally rotated and visibly shortened. The robot’s acoustic sensors pick up a high-frequency “pain moan” which the AI tags as a priority vocalization.
The RN activates a “Clinical 911” link. Rather than a standard emergency call, the RN transmits a “Digital Triage Pack”—including the video of the fall, a summary of the suspected fracture, and 10 minutes of real-time vitals—directly to the arriving EMS tablet. While waiting for the ambulance, the RN commands the robot to apply a built-in “Thermal Pack” to the injury site and coaches the patient through controlled breathing exercises via the robot’s speakers. In this scenario, the robot functions as a rigid medical stabilizer, a diagnostic transmitter, and a therapeutic bridge, significantly improving the “Golden Hour” of trauma response through nurse-led surrogate agency.
Ethical Considerations and Policy Requirements
The integration of embodied AI into the home necessitates rigorous ethical safeguards to prevent the “warehousing” of the elderly and the erosion of privacy.
Conclusion
The evolution of nursing in the era of AI and robotics is not a narrative of replacement, but one of professional elevation. By assuming the role of Clinical Systems Architects, Registered Nurses can leverage humanoid robots to provide a level of vigilance, physical safety, and diagnostic precision that human labor, by its biological nature, cannot sustain.
This hybrid model stabilizes the home care industry by eliminating the human capital trap—reducing churn, lowering liability, and ensuring 24/7 coverage. We must move beyond the sentimental attachment to manual labor and embrace a future where care is defined by its reliability and clinical outcomes. By transforming the “dirty, dull, and dangerous” tasks of geriatric care into an automated, data-driven process, we empower Registered Nurses to work at the absolute top of their license. This ensures that the most vulnerable members of society receive care that is both technologically superior and humanely governed, preserving the essence of nursing in an increasingly automated world.
References
Activated Insights. (2025). Benchmarking Report on Caregiver Turnover and Recruitment Costs.
Grand View Research. (2025). Elder Care Assistive Robots Market Size, Share & Trends Analysis Report, 2025-2033.
Locsin, R. C. (2005). Technological Competency as Caring in Nursing: A Model for Practice. Sigma Theta Tau International.
Peplau, H. E. (1952). Interpersonal Relations in Nursing. Putnam.
PHI. (2024). The State of the Direct Care Workforce: 2024 Data and Trends. Policy Research Report.
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026