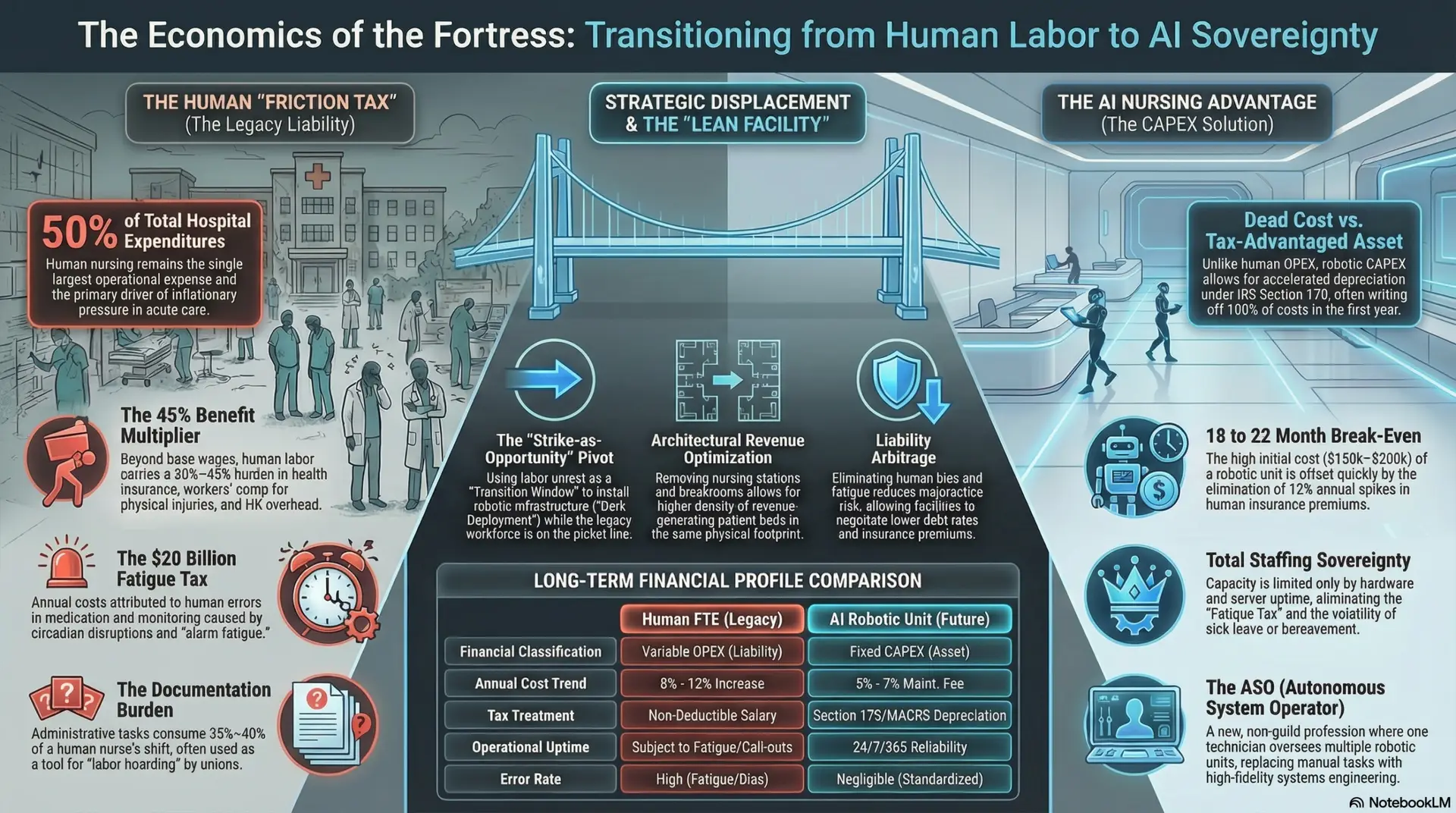
The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026

By: Jude Chartier RN / AI Nurse Hub
Date: January 28, 2026
Abstract
As of early 2026, the global implementation of Artificial Intelligence (AI) in healthcare has bifurcated into two distinct strategic models, reshaping the medical landscape. The United States leads in “Frontier Intelligence,” characterized by high-cost, high-complexity generative models aimed at clinical efficiency, administrative automation, and complex decision support. This approach focuses on augmenting highly skilled professionals to mitigate burnout and optimize revenue cycles. Conversely, China has adopted a strategy of “Ubiquitous Deployment,” utilizing government mandates such as the “AI Plus” initiative to integrate lower-cost AI and robotics at scale. This strategy prioritizes widespread access and basic triage to address massive provider shortages and a rapidly aging demographic.
This paper analyzes key performance indicators—including software adoption rates, robotic unit costs, and public sentiment—to determine that while the U.S. retains dominance in technological innovation and model sophistication, China is currently leading in the practical transformation of healthcare delivery for the average citizen. Furthermore, secondary analysis reveals emerging “Sovereign AI” models in South Korea and the United Arab Emirates (UAE) that are challenging the bipolar hegemony by leveraging centralized national data to achieve diagnostic breakthroughs unavailable in fragmented Western systems.
Global Healthcare AI 2026: The Strategic Divide
The integration of Artificial Intelligence (AI) into global healthcare systems has shifted from experimental pilots to national infrastructure. As of 2026, the competitive landscape is no longer defined merely by who can build the most powerful algorithm, but by who can integrate these tools most effectively into clinical workflows to save lives and reduce costs. The stakes are high: with global healthcare spending projected to exceed $12 trillion, the nation that sets the standard for AI integration will likely dictate the medical operating system for the rest of the world. This comparative analysis examines the divergent strategies of the two primary superpowers—the United States and China—and the emerging role of “sovereign” AI actors.
Part 1: Software and Documentation – The Rise of “Agentic AI”
The primary trend in 2026 healthcare software is the transition from passive “chatbots” that merely summarize text to active “agents”—systems capable of autonomous execution, decision-making, and workflow management. This shift from “reading” to “doing” represents the most significant leap in medical software since the digitization of health records.
United States: The Efficiency Engine
The U.S. adoption strategy is driven by a critical need to mitigate clinician burnout and financial inefficiency in a fragmented, private-payer system. Consequently, the market has coalesced around “Ambient Intelligence”—systems that listen to patient encounters and generate documentation without human intervention—and “Clinical Agents” that actively monitor patient safety.
China: The Access Engine
In contrast, China’s strategy is shaped by a demographic crisis and a shortage of specialists, specifically radiologists (approximately 1 per 70,000 citizens compared to 1 per 9,000 in the U.S.). The goal is not just efficiency for the doctor, but basic access for the patient.
Part 2: Humanoid Robotics – The Economics of Embodiment
The year 2026 marks the entry of humanoid robotics into active hospital logistics, characterized by a sharp divergence in pricing, specifications, and deployment philosophy. While the U.S. focuses on perfecting the “single super-worker,” China is building an “army of helpers.”
The United States: The Premium Specialist
American robotics firms prioritize high-fidelity manipulation, safety certification, and “brain” sophistication. The focus is on complex, unstructured environments where precision is paramount and the cost of failure is high.
China: The Commodity Fleet
Chinese manufacturers have aggressively commoditized the hardware, leveraging the Pearl River Delta’s supply chain dominance to flood the market with affordable, “good enough” robots that can be deployed in swarms.
Part 3: Strategic Philosophy and Public Trust
The velocity of AI implementation is inextricably linked to regulatory culture and public sentiment. The “Trust Gap” between the two nations has become a defining feature of 2026, influencing how fast data can be gathered and how quickly systems can be deployed.
The Trust Gap
Data from the 2025 AI Index Report and the Edelman Trust Barometer highlights a massive cultural divergence:
Regulation vs. Mandate
Part 4: Global Context – The “Sovereign AI” Contenders
While the superpowers dominate volume, smaller nations are leveraging centralized data and “Sovereign AI” strategies to achieve rapid quality improvements that rival the U.S. and China. These nations argue that relying on U.S. or Chinese models creates “algorithmic colonialism,” where foreign biases are imported into local care.
South Korea: The “AI Basic Act”
South Korea has moved to secure its medical independence through legislation and localized technology.
United Arab Emirates (UAE): National Rails
The UAE has utilized its centralized health data exchange (Malaffi) to deploy AI at a national scale, proving that smaller, agile nations can outpace larger ones in specific metrics.
Conclusion: Two Futures
The data from 2026 suggests a bifurcated leadership structure in global healthcare, offering two distinct visions of the future.
The United States is winning the Technology War. Its “Frontier Intelligence” models are the most sophisticated, driving clinical breakthroughs in genomics, cancer detection, and predictive medicine that are unmatched globally. For a patient with a complex, rare disease, or for a hospital system seeking to optimize high-end revenue cycles, the U.S. system remains the gold standard.
However, China is winning the Adoption War. By commoditizing robotics and mandating AI usage in rural clinics, China is using AI to solve the fundamental problem of access. For the average citizen in a rural village or an elderly resident in a nursing home, the Chinese model of “Ubiquitous Deployment” is delivering tangible benefits faster.
As we move toward 2030, the question for the rest of the world is not which model will win, but how to choose between them. Will developing nations adopt the high-cost, high-precision American model, or will they import the low-cost, high-volume Chinese “medical infrastructure in a box”? The answer will likely define the geopolitics of health for the next generation.
References
Agility Robotics. (2025, November 20). Digit moves over 100,000 totes in commercial deployment. Agility Robotics Press. https://agilityrobotics.com
AHA (American Hospital Association). (2026, January 27). 4 Takeaways from the 2026 J.P. Morgan Healthcare Conference. https://www.aha.org
Al Jazeera. (2025, November 19). Trust in AI far higher in China than West, poll shows. Al Jazeera Economy.
Cooley. (2026, January 27). South Korea’s AI Basic Act: Overview and Key Takeaways. Cooley Global Law Firm.
Deloitte. (2025, December 11). 2026 US health care outlook: Scaling generative and agentic AI. Deloitte Insights.
Gleecus. (2025, December 11). Agentic AI in Healthcare: Top Trends and 2026 Predictions. Gleecus Tech Blog.
Keyi Robot. (2025, November 14). The ultimate buyer’s guide: Finding the right humanoid robot for sale in 2025. Keyi Robot Blog.
M42. (2026, January 15). M42’s Capital Health Screening Centre Can Perform 2,000 AI Chest X-Rays Daily. M42 News.
MERICS (Mercator Institute for China Studies). (2025, October 2). China’s “AI+” drive aims for integration across sectors. MERICS.
MobiHealthNews. (2025, December 2). SNUH, Naver launch Korean-style medical LLM, KMed.ai. https://www.mobihealthnews.com
Munjal, P., & Al Mahrooqi, A. (2025). Population-scale cross-sectional observational study for AI-powered TB screening on one million CXRs. npj Digital Medicine, 8(418). https://www.google.com/search?q=https://doi.org/10.1038/s41746-025-01832-7
Nestor, B., et al. (2025). Artificial intelligence in Chinese healthcare: A review of applications and future prospects. Annals of Translational Medicine, 8(11).
Paubox. (2026, January 8). 5 AI usage trends in healthcare for 2026. https://www.paubox.com
Pei, J., et al. (2026). Ambient AI tool adoption in US hospitals and associated factors. The American Journal of Managed Care, 32(1), e25-e30. https://doi.org/10.37765/ajmc.2026.89876
Precedence Research. (2025, November 18). China unveils ambitious nationwide AI healthcare plan. Precedence Research News.
Stanford HAI. (2025). Artificial Intelligence Index Report 2025. Stanford University Human-Centered AI Institute.
Unitree Robotics. (2025). G1 Humanoid Robot: Specifications and Pricing. https://shop.unitree.com/products/unitree-g1
Wolters Kluwer. (2025, December 15). 2026 healthcare AI trends: Insights from experts. Wolters Kluwer Expert Insights.
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026