The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub
Date: March 2, 2026
Abstract
As healthcare systems integrate Artificial Intelligence (AI) and robotics at an unprecedented rate, a significant “preparedness-impact gap” has emerged among the frontline nursing workforce. While technology promises to alleviate administrative burdens and enhance patient safety, success is contingent upon nursing AI literacy. This article explores the core competencies of AI literacy, addresses the psychological roots of technological reluctance, and quantifies the Return on Investment (ROI) for healthcare organizations. Through the lens of the Diffusion of Innovation theory, we examine how a structured investment in human capital—specifically the working nurse—is the primary driver of digital transformation success. This expansion further investigates the role of “technostress,” the shift toward augmented clinical reasoning, and the long-term socio-economic implications of a digitally fluent nursing workforce.
Introduction: The Dual Burden of Modern Nursing
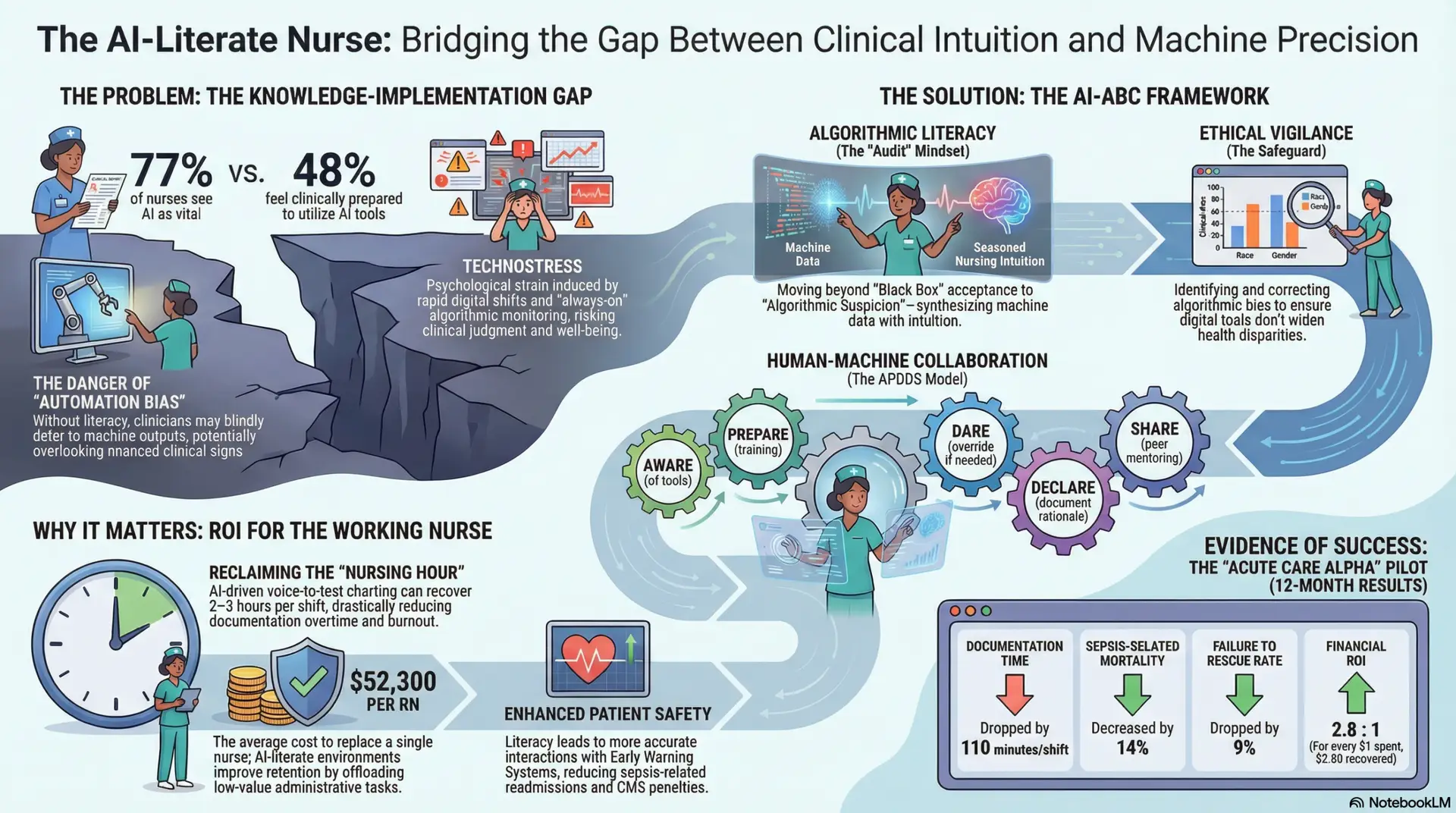
By early 2026, the integration of Artificial Intelligence in clinical settings has transitioned from a progressive luxury to an operational mandate. Current industry data suggests that while approximately 77% of nurses recognize AI as a vital component of the future of healthcare, fewer than half feel prepared to utilize these tools in a clinical capacity (Wolters Kluwer, 2025). This discrepancy represents a critical vulnerability in the healthcare infrastructure, often referred to as the “Knowledge-Implementation Gap.”
To ensure patient safety and workforce sustainability, AI literacy must be repositioned not as a technical “extra,” but as a core clinical competency on par with advanced life support certifications. For the modern nurse, the burden is no longer solely clinical; it is a dual burden of managing complex human pathologies while simultaneously navigating intricate digital landscapes. Furthermore, the introduction of “technostress”—the psychological strain induced by rapid digital shifts and the “always-on” nature of algorithmic monitoring—necessitates a proactive educational framework to maintain clinical judgment and staff well-being (Frontiers in Digital Health, 2025). Without this framework, healthcare systems risk high rates of “automation bias,” where clinicians defer blindly to machine outputs, potentially overlooking nuanced clinical signs that a computer cannot yet perceive.
The Three Pillars of Nursing AI Literacy: The AI-ABC Framework
To effectively lead in an augmented environment, working nurses must master three specific domains of literacy to ensure that technology serves the patient rather than dictates the care (Nursing Outlook, 2025). This mastery allows the nurse to act as a “digital translator,” converting machine data into compassionate care plans.
1. Algorithmic Literacy (The “Audit” Mindset)
This involves moving beyond “Black Box” acceptance to “Algorithmic Suspicion.” Nurses must understand the underlying logic of predictive models to identify when a machine’s risk score contradicts clinical reality. For example, a sepsis prediction tool might flag a patient based on tachycardia, failing to account for the fact that the patient just returned from physical therapy. Literacy in this domain involves “augmented clinical reasoning,” a synthesis of empirical machine data and the nurse’s seasoned intuition (International Journal of Medical Informatics, 2024). Nurses must be trained to ask: What data points fed this recommendation, and do they align with the patient’s current physical presentation?
2. Ethical Vigilance: Protecting the Vulnerable
Nurses serve as the final ethical safeguard against algorithmic bias. AI models are trained on historical data, which often contains systemic biases regarding race, gender, and socioeconomic status. Literacy includes the ability to recognize when datasets may penalize patients based on these factors, ensuring that digital tools do not inadvertently widen health disparities (American Nurses Association [ANA], 2024). This requires a deep understanding of “Social Determinants of Health” (SDOH) and how they intersect with digital health records. If an AI suggests a lower priority for a patient because they lack a history of consistent primary care, the AI-literate nurse must advocate for that patient, recognizing the systemic barriers rather than accepting the machine’s “neutral” assessment.
3. Human-Machine Collaboration (The APDDS Framework)
Utilizing frameworks such as APDDS (Aware, Prepare, Dare, Declare, Share), nurses must shift from being passive end-users to active auditors. This transition is essential for maintaining the “human-in-the-loop” requirement necessary for high-stakes medical decision-making (Computers, Informatics, Nursing [CIN], 2024).
Addressing Technological Reluctance: The “Late Majority” Challenge
A significant challenge in the digital transformation of nursing is the psychological reluctance found in a portion of the workforce—estimated between 30% and 45% (Rogers, 2003). This resistance is rarely age-specific; rather, it stems from a fundamental aversion to change, fear of surveillance, or the perceived “dehumanization” of care. This “Late Majority” often feels that technology is an intruder in the sacred space between nurse and patient.
According to the Diffusion of Innovation (DOI) theory, these adopters require specific strategies to move toward acceptance (Rogers, 2003):
Quantifying the ROI: The Financial and Qualitative Case for Training
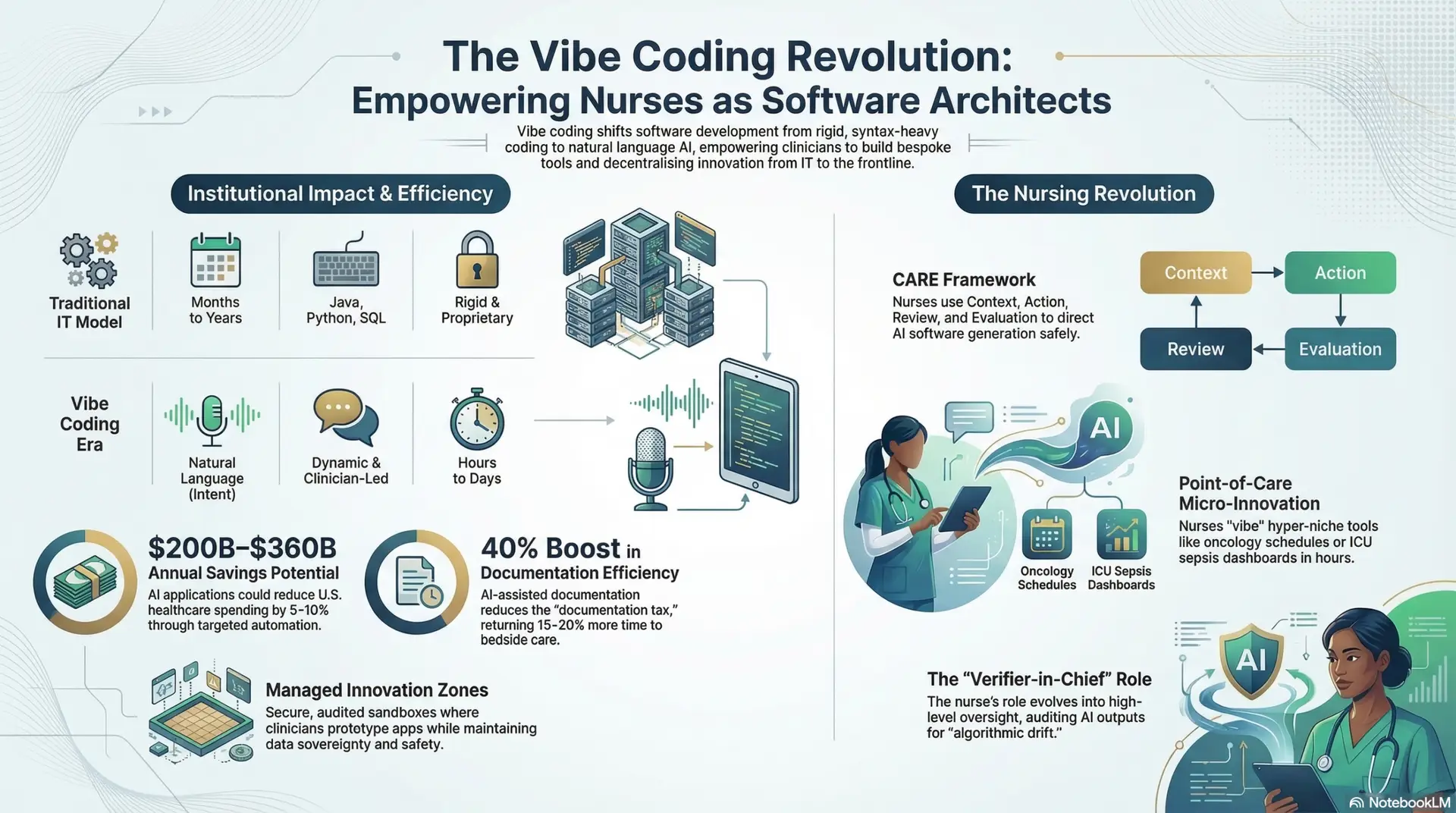
The implementation of AI literacy training requires a significant investment—typically ranging from $1,000 to $3,000 per nurse (MIT Project NANDA, 2025). While this upfront cost can be daunting for hospital administrators, the long-term ROI is multi-dimensional.
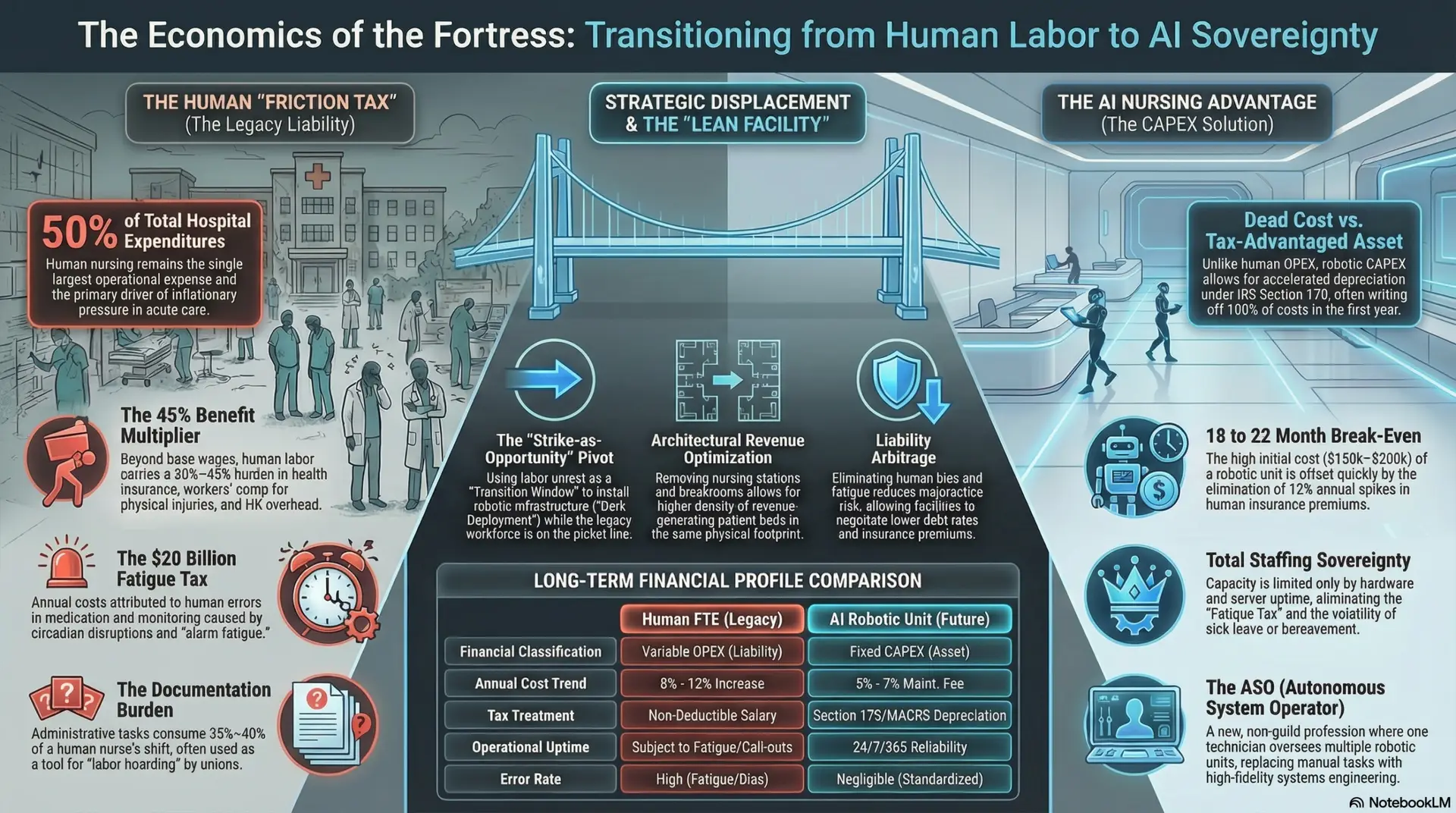
1. Operational ROI: Reclaiming the Nursing Hour
Ambient Clinical Intelligence (ACI), or voice-to-text charting, is perhaps the most immediate driver of ROI. By allowing nurses to dictate notes in real-time or having AI “listen” to patient interactions to draft assessments, facilities can recover 2–3 hours per shift for a bedside nurse. In a standard 500-bed facility, this recovers thousands of hours of nursing capacity annually, directly reducing the reliance on expensive agency staffing and decreasing the frequency of “documentation overtime” (CIN, 2024).
2. Retention and Moral ROI: Combatting the “Great Resignation”
By offloading repetitive, low-value administrative tasks to AI, nurses report higher job satisfaction and lower levels of “moral distress”—the feeling of being unable to provide the care they know is needed due to time constraints. Reducing nurse turnover by even 10% can save a facility millions. The cost of replacing a single RN in 2026 averages $52,300, which includes recruitment, onboarding, and the “lost productivity” of the orientation period (Premier Inc., 2025). Furthermore, AI-literate environments attract high-quality new graduates who seek out “digitally mature” institutions.
3. Clinical ROI and HCAHPS Scores
AI-literate staff more accurately interact with Early Warning Systems (EWS), leading to a marked reduction in sepsis-related readmissions and the associated CMS penalties (Premier Inc., 2025). Additionally, when nurses spend less time at a computer and more time at the bedside, patient satisfaction scores (HCAHPS) naturally rise. Every point increase in HCAHPS scores can trigger significant incentive payments from payers, creating a “virtuous cycle” of clinical excellence and financial health.
Case Study: The “Acute Care Alpha” Pilot (2025)
Setting: A 450-bed metropolitan hospital facing high burnout rates, a 22% RN turnover, and increasing “Failure to Rescue” incidents.
Intervention: The facility invested $1.2 million in a comprehensive “AI-ABC” certification program for its 600 staff nurses. The training was not merely a software tutorial; it was a clinical immersion into the ethical auditing of predictive sepsis alerts and the use of ACI for documentation.
Results (12 Months Post-Implementation):
Conclusion: The Human Compass in a Digital Sea
The evolution of nursing in the era of AI is not a story of machines replacing humans; it is a story of machines requiring more highly skilled humans to act as their moral and clinical compass. The “Human Touch” is not a static concept; it must evolve to include the ability to navigate digital systems with grace and skepticism. By investing in AI literacy, healthcare leaders do more than improve their bottom line—they empower their most valuable asset, the working nurse, to provide care that is both technologically advanced and deeply human. In the final analysis, the most sophisticated algorithm in the hospital is still the nurse’s ability to look into a patient’s eyes and know exactly what they need.
References
Allam, A., Shadhin, S., & Crockett, P. (2025). Explainable AI in clinical pathways: A guide for nursing leadership. Shadhin Lab Publications.
American Nurses Association. (2024). Position statement: The ethical use of artificial intelligence in nursing practice. https://www.nursingworld.org
Frontiers in Digital Health. (2025). Technostress and digital health literacy: A systematic review of the 2024–2025 nursing workforce.
https://www.google.com/search?q=https://doi.org/10.3389/fdgth.2025.00123
International Journal of Medical Informatics. (2024). Augmented clinical reasoning: The role of the nurse as an algorithmic auditor. https://www.google.com/search?q=https://doi.org/10.1016/j.ijmedinf.2024.105421
Journal of Nursing Management. (2025). The economics of retention: How AI-driven workflows reduce turnover in acute care settings. https://www.google.com/search?q=https://doi.org/10.1111/jonm.13982
MIT Project NANDA. (2025). The economic impact of generative AI in hospital operations: A multi-year analysis. MIT Press.
Nursing Outlook. (2025). Building AI literacy with the AI-ABCs framework: A longitudinal study of nursing competency.
https://www.google.com/search?q=https://doi.org/10.1016/j.outlook.2025.01.005
Premier Inc. (2025). Redefining ROI in healthcare: A new framework for digital transformation and CMS compliance. https://www.google.com/search?q=https://www.premierinc.com/reports
Rogers, E. M. (2003). Diffusion of innovations (5th ed.). Free Press.
Wolters Kluwer. (2025). The future of nursing with AI: Where the profession stands in a new era. https://www.google.com/search?q=https://www.wolterskluwer.com/en/health/nursing-ai-report
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026