The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub
Date: February 18, 2026
Abstract The integration of autonomous AI agents and embodied robotics into acute care settings represents a paradigm shift from assistive technology to agentic partnership. This article explores the current trajectories of “Agentic AI”—systems capable of independent planning, reasoning, and multi-step execution—and their synergy with physical robotic platforms. We argue that this technological convergence will automate 60–80% of routine nursing tasks, necessitating a fundamental redefinition of the nursing role. By analyzing the impact on the “Science of Nursing” (empirical data and clinical outcomes) and the “Art of Nursing” (aesthetic, ethical, and personal knowing), we propose a “Clinical Director” model for future nursing practice. This evolution suggests that while the manual workload of nursing may diminish, the cognitive and ethical demands of clinical oversight will intensify, requiring a new set of competencies for the 21st-century nurse.
Introduction: The Advent of the Agentic Era
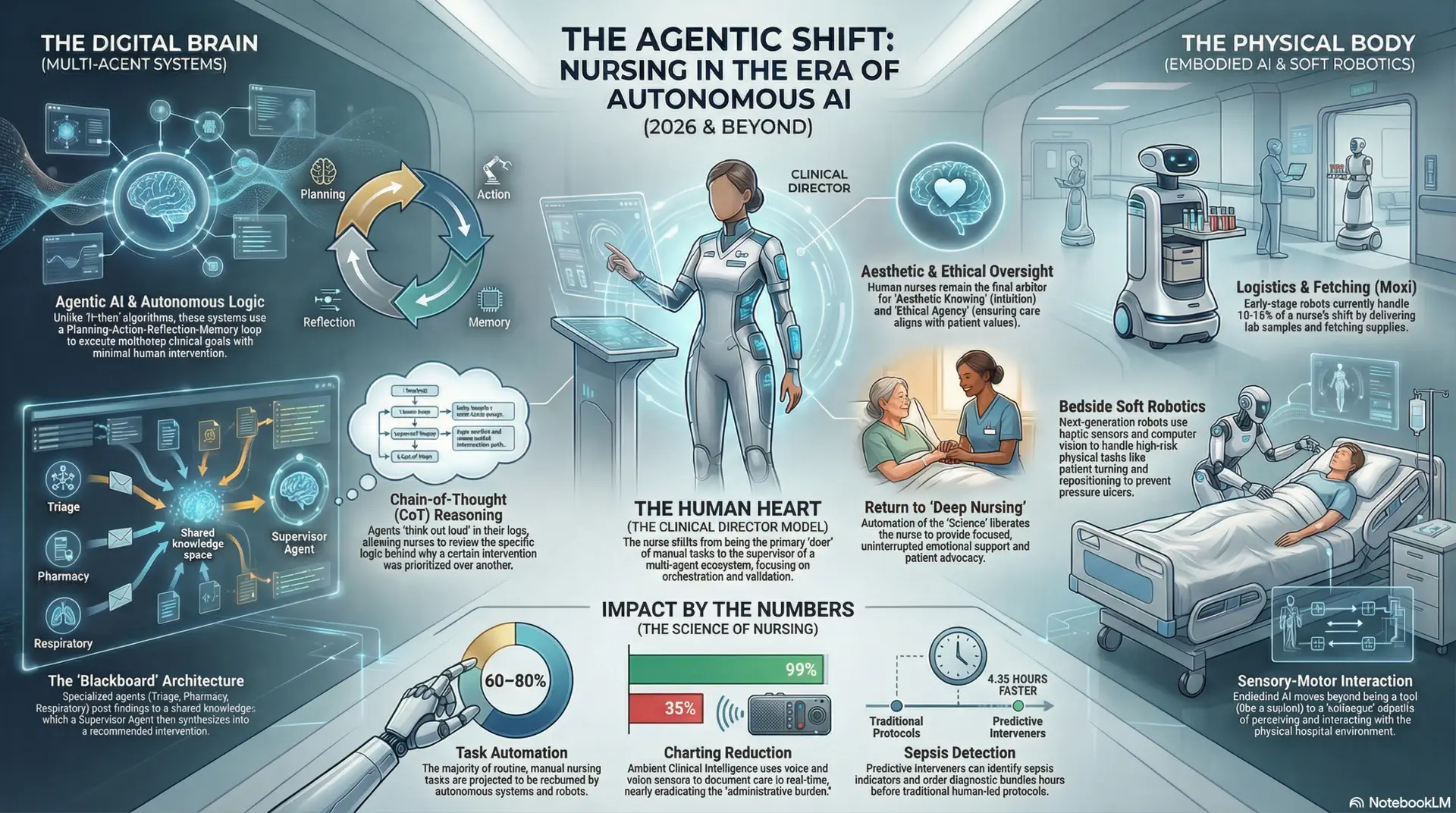
For decades, artificial intelligence in healthcare has been predominantly “passive” or “assistive,” serving as diagnostic support or data visualization tools. These systems operated on “if-then” logic or predictive modeling that required a human to interpret the output and initiate an action. However, current trajectories in Large Action Models (LAMs) and Multi-Agent Systems (MAS) are ushering in the era of Agentic AI (Cao et al., 2026). Unlike traditional algorithms that require specific prompts, autonomous agents possess a “Planning-Action-Reflection-Memory” loop that allows them to pursue complex clinical goals with minimal human intervention (PMC12629813, 2025).
In the high-acuity environment of the modern hospital, this shift is further amplified by Embodied AI—robotics capable of perceiving and interacting with the physical world through sensory-motor loops (Liu et al., 2025). We are moving beyond the “robot as a tool” (like a scalpel) to the “robot as a colleague” (like an assistant). The synergy between the “digital brain” (software agents) and the “physical body” (embodied robots) is poised to transform nursing from a labor-intensive profession defined by manual tasks to one of high-level clinical oversight and orchestration.
Architectural Models of Autonomous Intelligence
The functionality of autonomous agents in nursing is grounded in sophisticated architectural frameworks that allow for a level of reasoning previously reserved for human clinicians.
Multi-Agent Systems (MAS) and Blackboard Architectures
Modern nursing agents do not operate as a single monolithic program but within a Multi-Agent System, where specialized sub-agents collaborate to achieve a patient-centered goal (Deloitte, 2025). These systems utilize a “Blackboard” architecture, a shared knowledge space where different specialized agents “post” their findings and hypotheses.
For example, when a patient’s oxygen saturation dips:
Reinforcement Learning from Clinical Feedback (RLCF) and Chain-of-Thought Reasoning
The intelligence of these agents is dynamic. Using Reinforcement Learning (RLCF), agents learn to optimize care plans by interacting with real-world clinical feedback. If an agent suggests a specific weaning protocol for a ventilator and the patient’s vitals stabilize faster, the agent “learns” this as a successful strategy (Generated Health, 2026). Furthermore, these agents employ Chain-of-Thought (CoT) reasoning, allowing them to “think out loud” in their logs. A nurse can review the agent’s logic—seeing exactly why it prioritized a lab draw over a medication dose—which is critical for building the trust necessary for true autonomy.
The Science of Nursing: Operational and Clinical Metamorphosis
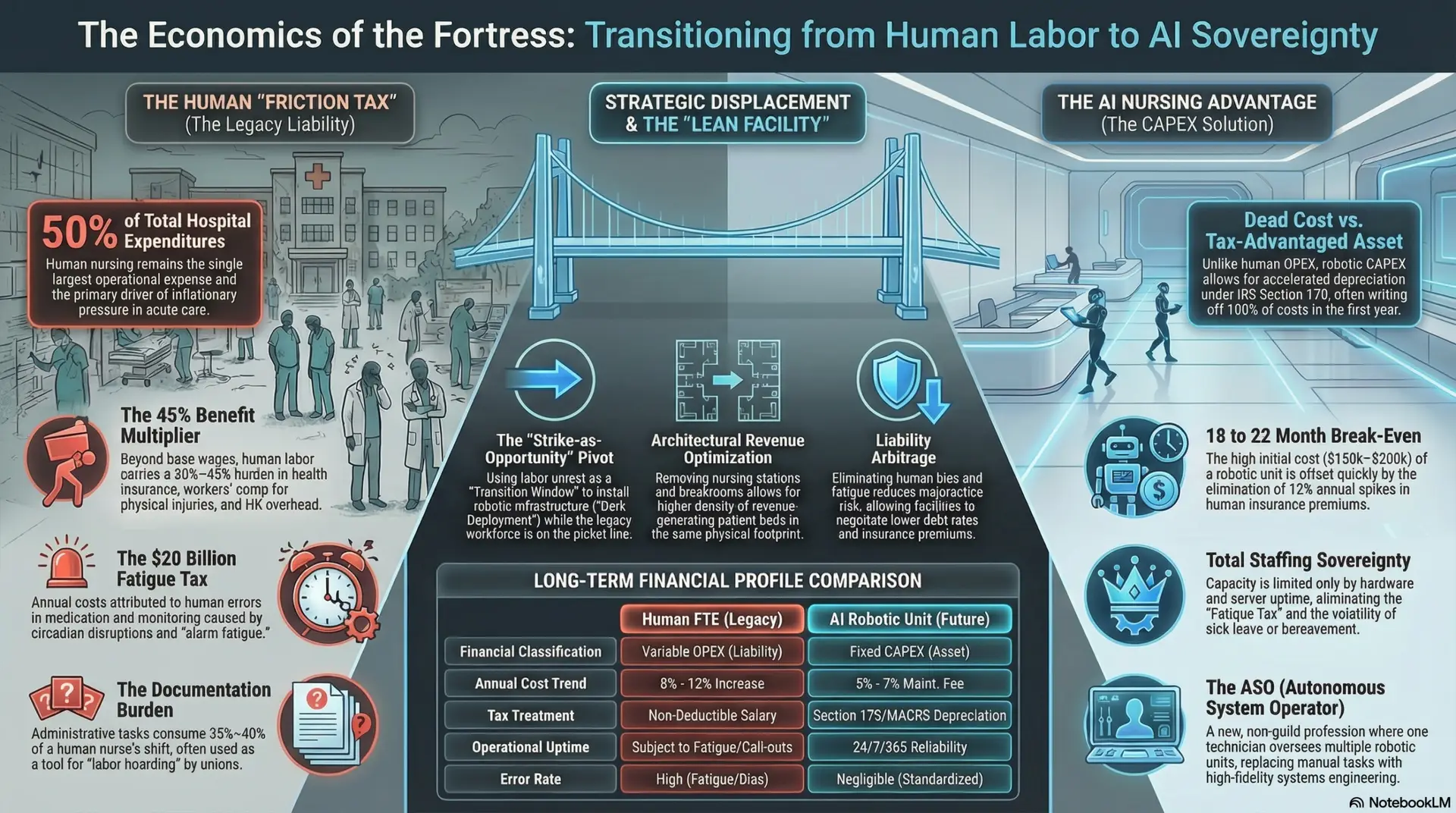
The “Science of Nursing” focuses on the empirical, measurable aspects of care—the data-driven interventions that lead to positive patient outcomes. Autonomous agents are projected to reclaim up to 80% of a nurse’s shift by addressing two primary burdens: cognitive load and physical labor.
Cognitive and Administrative Eradication
Traditional nursing involves significant “cognitive switching”—the mental tax of jumping between charting, paging doctors, and reviewing protocols. Autonomous agents eliminate this by providing Ambient Clinical Intelligence. Through secure voice and video sensors, agents can document a dressing change or a patient interview in real-time, reducing charting time by 35% to 99% (JKANA, 2026).
Beyond charting, these agents act as Predictive Interveners. In intensive care settings, AI agents have demonstrated the ability to detect sepsis indicators up to 4.35 hours earlier than standard human-led protocols. Because they can autonomously order “pre-approved” diagnostic bundles (like blood cultures and lactate levels), the time to treatment is slashed, directly impacting mortality rates (PMC12701216, 2025).
The Physical Revolution: Embodied AI and Soft Robotics
While software agents manage the data, embodied robots handle the physical logistics. Current data suggests that early-stage robots like Moxi can handle 10-15% of a nurse’s shift spent on “non-value-added” tasks like fetching supplies or delivering lab samples (arXiv:2602.03054, 2026).
However, the next generation of Embodied AI utilizes “Soft Robotics” and haptic sensors to assist with direct patient care. Tasks such as patient turning and repositioning—vital for preventing pressure ulcers but a leading cause of back injuries in nurses—can be performed by autonomous bedside units. These robots use computer vision to ensure the patient is positioned exactly according to the clinical protocol, maintaining a precision that is often difficult to achieve during a busy human shift.
The Art of Nursing: Preserving the Human Connection
A critical scholarly concern is whether autonomous agents will “dehumanize” care. If a robot performs the bed bath and a software agent handles the charting, what remains for the nurse? The answer lies in the Art of Nursing—the aesthetic, ethical, and personal ways of knowing.
By automating the “science” (the tasks), we allow the nurse to return to “Deep Nursing”—the focused, uninterrupted time for patient advocacy and emotional support that is currently sacrificed to the “altar of documentation.”
The “Clinical Director” Model: A Day in the Life
As task-oriented nursing fades, the Clinical Director model emerges. In this role, the nurse is no longer the primary doer of manual tasks but the supervisor of a multi-agent ecosystem.
Future of Nursing Education and Policy
The transition to agentic AI requires a radical overhaul of nursing education and regulatory policy.
Conclusion: Navigating the Trajectory
The integration of autonomous AI agents into acute care is not merely an upgrade to existing tools; it is a fundamental shift in the nursing identity. While 60–80% of current tasks may be automated, the professional responsibility of the nurse will arguably increase, shifting toward high-stakes clinical reasoning and the preservation of the human-patient bond in an increasingly automated environment.
The trajectory is clear: the future of nursing is a hybrid model. It is a world where the efficiency of the Silicon Agent, the physical endurance of the Embodied Robot, and the ethical wisdom of the Human Nurse converge. This synergy will not replace the nurse; rather, it will finally liberate the nurse to practice at the very top of their license, focusing on the complex, beautiful, and profoundly human work of healing.
References
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026