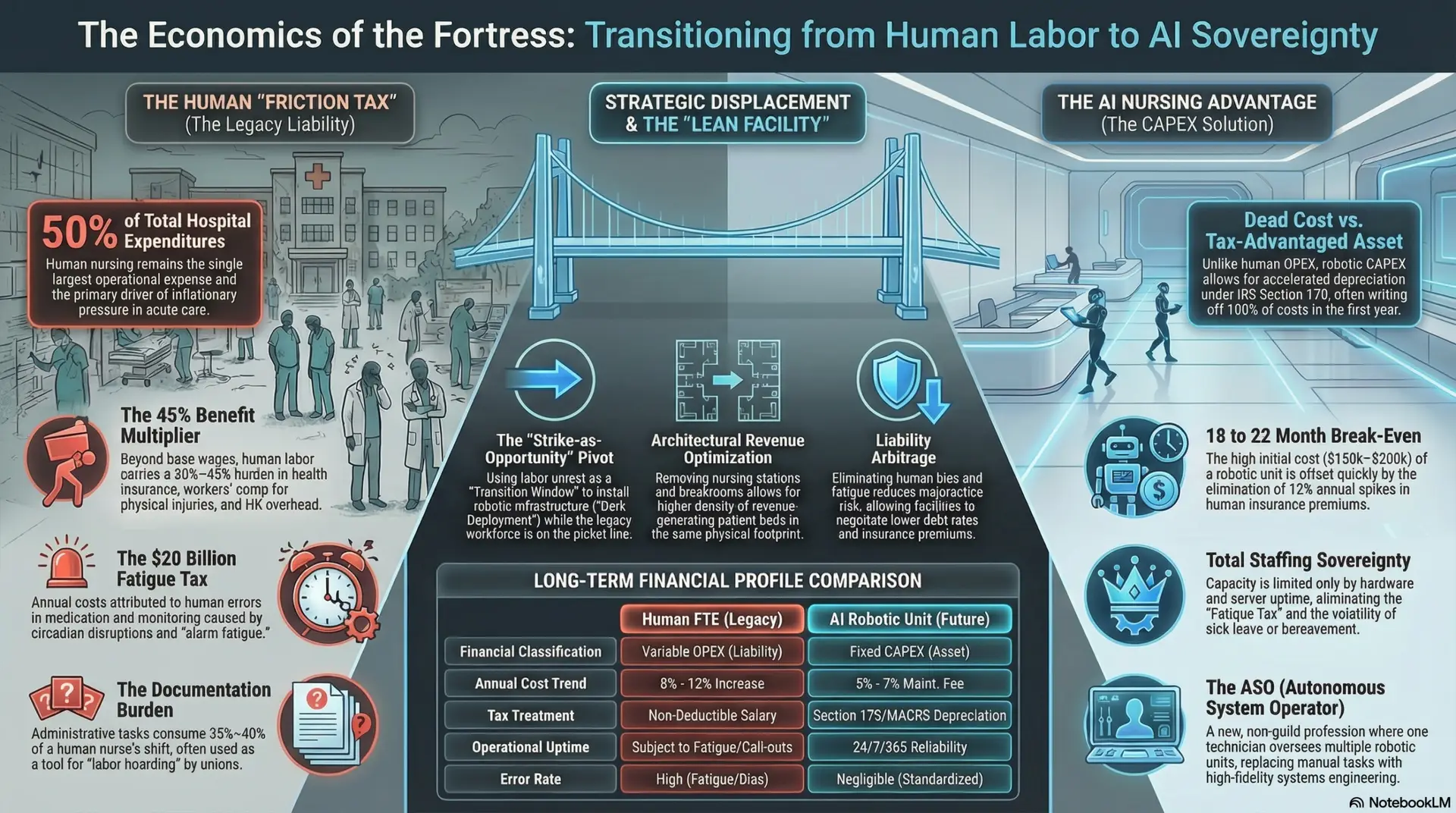
The Economics of the Fortress: Breaking Institutional Friction in Nursing
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026

By: Jude Chartier RN / AI Nurse Hub
Date: February 16, 2026
Abstract
The nursing profession currently navigates a dual crisis: a widening faculty shortage that limits instructional bandwidth and a clinical placement bottleneck that severely restricts student exposure to diverse patient populations and complex care environments. This article explores the evolution of “Nursing Education 2.0,” a transformative era characterized by the integration of artificial intelligence (AI) and immersive virtual simulations. By examining hyper-personalized learning pathways, conversational virtual reality (VR), and automated skill assessments, this paper evaluates the efficacy of AI-driven pedagogy in preparing students for the modern healthcare landscape. Crucially, it addresses the burgeoning debate: Can AI virtual simulations replace hands-on clinical hours? The findings suggest that while AI provides a superior, psychologically safe environment for repetitive mastery and cognitive development, it serves as a sophisticated bridge rather than a total replacement for the human-centric nuances, sensory complexities, and unpredictable nature of bedside care.
Introduction
The transition from the controlled environment of a nursing student to the high-stakes responsibility of a registered nurse is often marked by “clinical shock.” This phenomenon occurs when the high-pressure reality of hospital environments—characterized by rapid-fire decision-making, multifaceted patient loads, and emotional intensity—overwhelms the foundational knowledge and technical skills gained in the classroom. Traditionally, high-fidelity simulation (HFS) using static mannequins has been the gold standard for bridging this gap. However, these traditional methods are often limited by scripted scenarios and the inability to replicate the fluid, conversational nature of human interaction. As Buchanan et al. (2024) observe, the advent of artificial intelligence (AI) is ushering in a paradigm shift toward more dynamic, pedagogical models that adapt to the learner in real-time.
The central challenge in modern nursing education is ensuring that students are truly “practice-ready” in an era where clinical complexity is rising alongside patient acuity. AI offers a potential solution through hyper-personalized learning pathways, immersive conversational simulations, and objective clinical feedback. However, as these technologies advance and the fidelity of virtual environments begins to rival reality, educators and regulatory bodies must grapple with a critical question: Could AI virtual simulations eventually replace actual hands-on clinical hours? This article argues that while AI significantly enhances clinical judgment and technical proficiency by allowing for thousands of “digital repetitions,” its primary value lies in fostering a more confident workforce through safe failure. It acts as a mandatory precursor—but not a total substitute—for the multisensory human bedside experience.
Hyper-Personalized Learning: The AI Clinical Tutor
One of the most transformative aspects of AI in education is the departure from linear, one-size-fits-all curricula. Traditional nursing education often forces a diverse group of learners through a static timeline, regardless of individual mastery levels. In contrast, adaptive learning systems utilize sophisticated algorithms to adjust the difficulty and type of content based on the individual student’s real-time performance (Liu et al., 2025). For instance, a student struggling with the pharmacological nuances of cardiac medications, such as beta-blockers or ACE inhibitors, will be served targeted remediation, case studies, and quiz questions that focus specifically on those mechanisms. Simultaneously, a student who demonstrates mastery in pharmacology can be automatically progressed to more complex diagnostic reasoning or multi-system failure scenarios.
Furthermore, AI-driven predictive analytics are now being utilized as an early warning system to ensure licensure success. By analyzing massive datasets of historical student performance and longitudinal progress, AI models can identify students at risk of failing the NCLEX-RN months before they even graduate (Hwang et al., 2025). These models look beyond mere test scores, analyzing study habits, time spent on specific modules, and even the “confidence” indicated by the speed of their answers. This allows faculty to implement early, data-driven interventions, such as intensive coaching or personalized study plans, which support student retention and success. Effectively, AI acts as a 24/7 personal tutor that ensures no cognitive gaps remain unaddressed before a student enters a clinical setting, thereby maximizing the efficiency of their precious clinical hours.
Conversational AI and Virtual Reality (VR)
The integration of Natural Language Processing (NLP) into Virtual Reality has solved a long-standing limitation of simulation: the “silent” or “scripted” patient. Historically, a student in a simulation lab would have to “suspend disbelief” as an instructor spoke through a mannequin from a control booth. Modern VR simulations, powered by Large Language Models (LLMs), allow students to engage in dynamic, non-scripted dialogue with virtual patients who possess unique personalities, medical histories, and emotional states (Liaw et al., 2025). This technology assesses not just the clinical accuracy of a student’s response—such as asking the right diagnostic questions—but also their “soft skills.” It can track the student’s tone, the use of therapeutic communication techniques, and the ability to de-escalate an anxious or frustrated patient in real-time.
These simulations are particularly vital for “High-Acuity, Low-Frequency” (HALF) scenarios. In traditional clinical rotations, the luck of the draw determines a student’s exposure; one student may spend an entire semester without witnessing a pediatric cardiac arrest or a rare, life-threatening transfusion reaction. AI-driven VR provides safe, repeatable exposure to these high-stakes emergencies. Students can “manage” a virtual code blue a dozen times until the protocols are etched into their muscle memory. The implications are profound: when these events occur in real life, the nurse’s response is governed by practiced competence rather than the paralyzing effects of panic. This level of readiness simply cannot be guaranteed by traditional clinical rotations alone, where patient safety often limits student involvement in critical interventions.
The Digital Preceptor: Objective Skill Assessment
The “skills lab” has traditionally been a bottleneck in nursing programs, often plagued by grading inconsistency due to human instructor bias, fatigue, or varying interpretations of subjective rubrics. The emergence of the “Digital Preceptor”—a system utilizing computer vision, haptic sensors, and AI—offers a rigorous solution. These systems provide real-time, objective feedback on manual dexterity tasks that require high precision. For example, when a student is practicing the insertion of a Foley catheter, the AI can track the exact movements of their hands to detect if a sterile field was breached, even by a millimeter. Similarly, during CPR training, sensors can provide a “heat map” of compression depth, recoil, and rate, giving the student instant, actionable data to improve their performance.
By comparing traditional instructor evaluations with AI-driven data, institutions can ensure a standardized level of competency across the entire student body (Blank, 2025). This technology also allows for “on-demand” learning. Rather than waiting for an instructor to be free to sign off on a skill, a student can practice independently with the AI preceptor, receiving high-fidelity feedback at 2:00 AM if they choose. This democratization of feedback accelerates skill acquisition and ensures that every student meets the same high standard of patient safety before they ever touch a human being.
Discussion: Replacement vs. Augmentation
The question of whether AI simulations can replace hands-on clinical hours is a subject of intense debate among nursing regulatory bodies and state boards of nursing. The landmark NCSBN Simulation Study previously suggested that up to 50% of clinical hours could be replaced by high-quality simulation without compromising student outcomes or safety. With the advent of AI, the fidelity, complexity, and psychological realism of these simulations have increased exponentially, leading some to argue for even higher replacement ratios. Proponents of replacement argue that virtual environments are more “fair” and “comprehensive,” ensuring every student encounters the same set of critical scenarios, whereas traditional clinicals are often “hit or miss.”
However, clinical nursing is not merely the sum of technical tasks, diagnostic algorithms, and verbal communication. It involves what veteran nurses often call the “nursing gut”—a complex, multi-sensory perception of a patient’s changing condition. A machine can simulate a drop in blood pressure, but it cannot yet replicate the specific smell of a GI bleed, the subtle change in skin turgor or temperature, or the intuitive feeling a nurse gets when a patient “just doesn’t look right” despite stable vitals. Furthermore, the unpredictable nature of a chaotic hospital ward—the interruptions from family, the coordination with a multidisciplinary team, and the physical exhaustion of a twelve-hour shift—is difficult to fully replicate in a virtual headset. Therefore, the “Human-in-the-Loop” remains an essential component of professional identity formation. AI should be viewed as a tool that allows students to reach a high baseline of technical and cognitive competency before they touch a patient, thereby making the actual hands-on hours more meaningful, focused on higher-level synthesis and human connection rather than basic skill acquisition.
Conclusion
Artificial intelligence is not a threat to the traditional nursing educator but a powerful ally that can alleviate the burden of repetitive instruction and subjective grading. By providing a psychologically safe environment for repetitive mastery, AI allows students to fail, learn, and try again without the catastrophic consequences of real-world error. While AI virtual simulations offer unprecedented opportunities for training in a diverse, risk-free environment, they are best utilized as a robust, mandatory bridge to clinical practice rather than a total replacement. The future of Nursing Education 2.0 lies in the purposeful synergy of machine precision and human compassion. By offloading the cognitive “grunt work” of drills and data analysis to AI, educators can focus on what a machine can never replicate: the development of deep mentorship, ethical reasoning, and the profound human connection that sits at the heart of the nursing profession.
References
American Association of Colleges of Nursing. (2021). The essentials: Core competencies for professional nursing education. https://www.aacnnursing.org/essentials
Blank, A. (2025). Active performance evaluation in the clinical setting (APECS): A tool for nursing education. University of Texas School of Nursing.
Buchanan, C., Howitt, M. L., Wilson, R., Booth, R. G., Risling, T., & Bamford, M. (2024). Predicted influences of artificial intelligence on the domains of nursing: Scoping review. JMIR Nursing, 7(1), e51093.
https://www.google.com/search?q=https://doi.org/10.2196/51093
Hwang, G. J., Tang, K. Y., & Lin, C. J. (2025). Trends in artificial intelligence supported nursing education: A systematic review. Nurse Education Today. [Advance online publication].
Liaw, S. Y., et al. (2025). Virtual reality simulation to teach communication for undergraduate nursing students: A scoping review. Journal of Advanced Nursing.
Author: Jude Chartier RN / AI Nurse Hub Date: March 30, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 23, 2026
By: Jude Chartier RN / AI Nurse Hub Date: March 19, 2026