By: Jude Chartier RN / AI Nurse Hub
Date: February 11, 2026
Abstract
In February 2026, the healthcare technology landscape reached a definitive inflection point as Epic Systems and athenahealth initiated the largest synchronized rollout of “agentic” artificial intelligence features in history. This transition marks the end of the Electronic Health Record (EHR) as a passive digital filing cabinet and its rebirth as an active clinical collaborator. This article provides a comprehensive analysis of the technical specifications of these updates, the resulting paradigm shift in the nursing profession, and the multi-dimensional return on investment (ROI) metrics—both fiscal and human—that are driving this rapid adoption. Furthermore, it addresses the burgeoning “accessibility gap,” where the uneven distribution of these tools across health systems threatens to create a new digital divide in clinical care and nursing equity.
Introduction: The Death of the Passive Record
As of early 2026, the nursing profession remains in a state of crisis, with burnout levels plateauing at historic highs. Retrospective studies from 2024 and 2025 consistently identified “documentation burden” as a primary driver of moral injury, with many bedside nurses spending nearly 35% of their active shift hours interfacing with a screen rather than a patient. The February 2026 updates represent a direct, algorithmic response to this crisis, moving beyond the simple “text generation” of early 2024 toward proactive, context-aware systems.
We have officially moved beyond “Generative AI”—which simply produces text based on prompts—into the era of “Agentic AI.” These systems are characterized by their ability to execute multi-step workflows, proactively queue data for verification, and interact with the physical environment via mobile sensors and ambient listening. This article explores how these agents are fundamentally altering the “transactional” nature of nursing documentation, shifting the burden of data entry from the human to the machine and redefining the professional identity of the Registered Nurse (RN).
Epic Systems: The ‘Art’ Suite and the Ambient Revolution
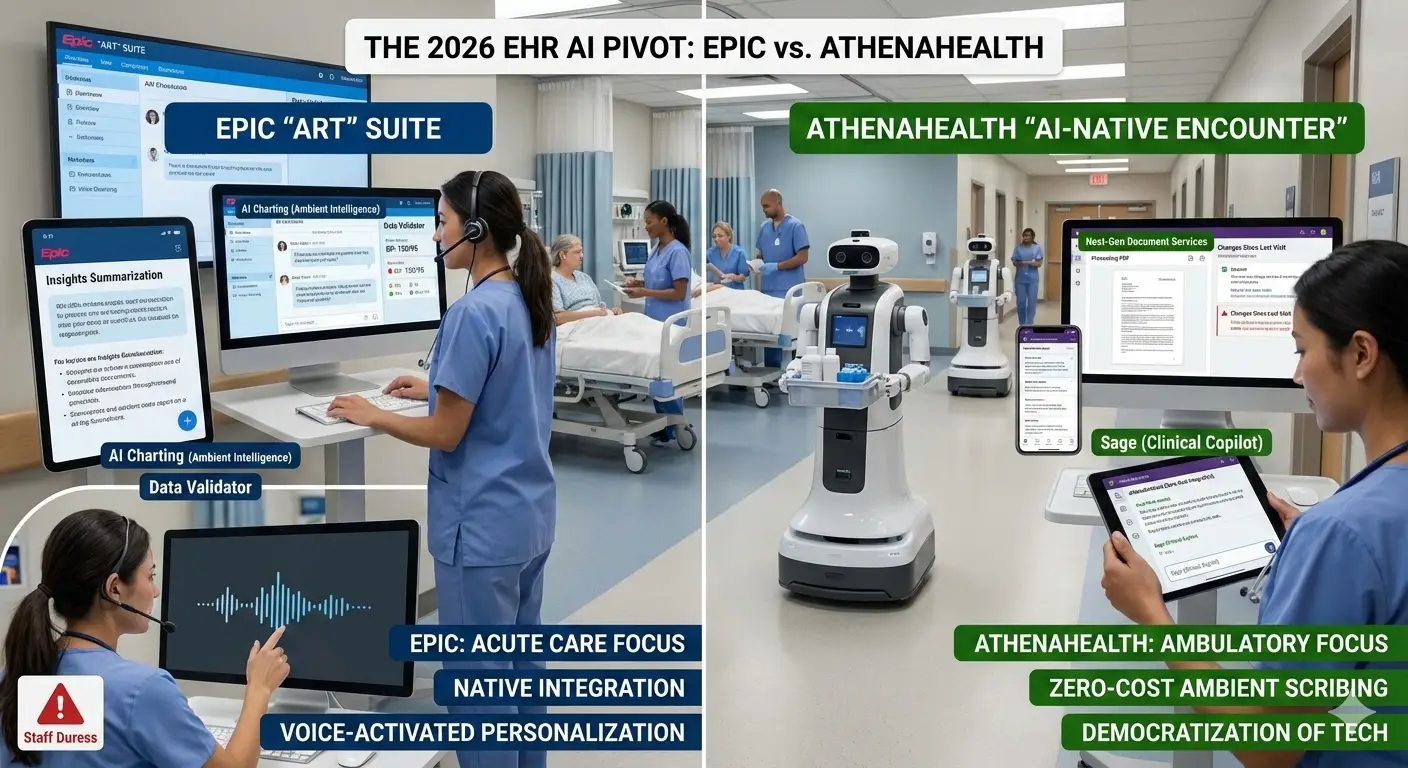
Epic’s February 2026 update is anchored by the Art (AI for Clinicians) suite. Unlike the fragmented, third-party “plug-ins” of previous years, Art is natively woven into the bedrock of Epic’s infrastructure, specifically targeting the Hyperspace desktop and Rover mobile environments. This native integration ensures that AI insights are not silos but integrated components of the patient’s longitudinal record.
Expanded Feature Deep-Dive for Epic (Feb 2026):
- AI Charting (Ambient Intelligence): This feature utilizes the advanced microphone arrays in modern mobile devices to distinguish between multiple voices in a patient room—filtering out television noise, family chatter, and machine alarms. It doesn’t just transcribe; it interprets. For example, if a nurse says, “Your blood pressure is a bit high today at 150 over 95,” the AI recognizes this as a discrete data point, cross-references it with the patient’s history, and automatically queues that value in the vitals flowsheet. The nurse’s role shifts from a data entry clerk to a Data Validator, where a single tap confirms the accuracy of the AI’s “suggestion.”
- Insights Summarization (The “Shift-Start” Agent): One of the most adopted features this month is a conversational search agent that acts as a digital handoff. It reviews the last 24–48 hours of progress notes, lab trends, and consultant recommendations to provide a 30-second “brief” for the nurse. By early February, Epic reported over 16 million summaries were being generated monthly. Beyond simple summaries, this agent flags “Actionable Gaps”—such as a missing wound care assessment or a late medication—helping nurses prioritize their first hour of care.
- Voice-Activated Personalization: Nurses can now manipulate the EHR interface using semantic commands, reducing the “menu-diving” that characterizes modern informatics. A nurse can say, “Epic, show me only the abnormal labs from the last three days and reformat the current assessment into a bulleted list for the surgical consult.” This “hands-free” interaction is particularly vital in sterile environments or during high-intensity procedures where manual computer interaction is impossible.
- Staff Duress APIs and RTLS Integration: In a significant move for workplace safety, Epic has integrated AI with Real-Time Location Systems (RTLS). If the AI detects specific acoustic keywords associated with aggression or if it observes a nurse remaining stationary in a high-risk zone for an unusual duration, it can automatically trigger a silent alert to security. This alert includes a “Pre-Alert Audio Buffer,” allowing security to hear the 30 seconds of audio preceding the alert to assess the severity of the threat.
- Emmie (The Patient-Facing Agent): While nurses focus on clinical care, the Emmie agent in MyChart handles the administrative friction that often falls back on nursing staff. Emmie can explain a complex bill in plain language, schedule follow-ups based on the nurse’s discharge instructions, and even guide patients through pre-op preparation checklists. This effectively “deputizes” the patient in their own care, reducing the volume of non-clinical calls to the nursing station by an estimated 22%.
athenahealth: The AI-Native Encounter and the Democratization of Tech
While Epic scales within the acute care sector, athenahealth’s February 2026 rollout focuses on the ambulatory and community health nurse. Their strategy is built on the “AI-Native Encounter”—a radical redesign that assumes AI is the primary user, with the human acting as the supervisor and final authority.
Expanded Feature Deep-Dive for Athena (Feb 2026):
- athenaAmbient (Zero-Cost Integration): Perhaps the most disruptive move in 2026 is Athena’s decision to include native ambient scribing in its standard updates at no additional cost. By removing the financial “paywall” that previously limited AI to elite health systems, Athena has enabled thousands of resource-strapped rural clinics to adopt AI overnight. This tool drafts HPIs, assessments, and plans in real-time, allowing nurses in fast-paced clinics to maintain eye contact with patients rather than staring at a laptop.
- Sage (The Clinical Copilot): Sage is a “cross-continuum” search engine. Unlike standard search bars, Sage understands clinical context. A nurse can query, “When was the last time this patient had an A1C above 7.0 across any facility we share data with?” Sage will traverse the ChartSync network, pull data from external hospitals via Interop APIs, and present a chronological trend line without the nurse ever leaving the current encounter.
- Next-Gen Document Services (Automated Intake): For clinics still plagued by paper, this AI reads incoming faxes and unstructured PDFs with 99.4% accuracy. It extracts discrete lab values, immunizations, and specialist notes, then maps them directly into reportable fields. This eliminates “Scanning Scavenger Hunts,” where nurses spend hours searching through PDFs for a single pathology result.
- “Changes Since Last Visit” (CSLV): This agentic feature proactively scans for any new diagnoses, meds, or hospitalizations that occurred since the patient was last seen at the clinic. It presents a “delta report” to the nurse during rooming. If a patient was hospitalized for heart failure between clinic visits, the CSLV agent flags this as the #1 priority for the current nurse assessment, ensuring no transitional care gaps go unnoticed.
The Accessibility Gap: The Governance and Infrastructure Barriers
The rollout of these features has exposed a growing disparity in the nursing experience. While the software is “available,” the ability to use it is filtered through the lens of organizational readiness and digital maturity.
- The Governance Barrier: Many large health systems have placed these AI features behind “Clinical Governance Boards” for 6-to-12-month reviews. These boards analyze “AI Hallucination Rates”—the frequency with which AI misinterprets a conversation—and the legal liability of AI-generated safety alerts. Consequently, a nurse at a tech-forward “Level 1” trauma center may have a completely different workflow than a nurse at a community hospital five miles away, leading to a “tech-equity” issue in nursing recruitment.
- The Hardware Hurdle: Ambient intelligence is only as good as the hardware supporting it. Facilities with aging Wi-Fi infrastructure or “dead zones” in lead-lined patient rooms find that the AI frequently disconnects, leading to a “tech-frustration cycle” where nurses spend more time troubleshooting the AI than they would have spent typing. This highlights that AI adoption is as much a civil engineering challenge as it is a software one.
- The “Shadow AI” Risk: When organizations delay the official rollout of secure, integrated AI, nurses often turn to personal, unvetted AI tools (like consumer LLMs) to summarize complex cases or draft patient education. This “Shadow AI” presents massive HIPAA and security risks, as patient data is often “leaked” into public training models. This creates an urgent imperative for hospitals: Provide a secure, official AI tool, or accept the risk of unvetted AI usage in your facility.
The Administrative Perspective: The Quantitative ROI Case
For hospital executives, the 2026 AI pivot is not just about staff morale; it is a financial necessity driven by tightening margins, value-based care mandates, and the escalating costs of labor.
Hard ROI: Revenue Cycle and Throughput
- The “Penny” Agent: Epic’s RCM agent, Penny, has fundamentally changed billing. By ensuring that nursing and physician documentation perfectly aligns with “Medical Necessity” requirements before the claim is even submitted, hospitals are seeing a 20% drop in initial denials. In a 500-bed system, this can represent upwards of $15 million in recovered annual revenue that previously sat in a “denials bucket.”
- Reduced Length of Stay (LOS): By using AI to automate discharge summaries—which traditionally take providers hours to compile—facilities are coordinating post-acute care placement much earlier in the day. This has led to a 0.5-day reduction in average LOS. This improves “throughput,” allowing hospitals to treat more patients without increasing physical bed capacity or capital expenditure.
Soft ROI: The Retention Economics
- The $60,000 Threshold: With the cost of replacing a single bedside RN now exceeding $60,000 (including recruitment, orientation, and “lost productivity” costs), reducing turnover by even 5% pays for the AI software license many times over.
- The Recruitment “AI Premium”: Administrators are now viewing AI as a “recruitment benefit,” similar to health insurance or 401k matching. New graduates are increasingly filtering employers based on technical support, asking during interviews, “Do you use ambient charting, or will I be doing manual entry?”
Clinical Implications and Ethical Safeguards: The “Nursing Editor” Role
The February 2026 rollouts signify the end of the “Data Entry” era of nursing. We are witnessing the birth of the Clinical Editor. In this new paradigm, the nurse’s primary value is not their ability to type fast or document every minute detail, but their ability to apply Nursing Judgment to the AI’s output.
The Risks of the AI Era:
- Automation Bias: The greatest clinical challenge of 2026 is “automation bias”—the tendency for a tired nurse to trust an AI-generated summary or vital sign without verification. If the AI “hears” 150/95 but the patient is actually 110/70, and the nurse clicks “Confirm” without checking, the clinical consequences can be dire.
- Loss of Narrative: There is a concern that AI-generated notes, while efficient, may lose the “nuance” of nursing care—the small observations about a patient’s mood or family dynamics that often signal a change in condition.
As we move forward, nursing education must shift from teaching how to document (the “what” and the “where”) to teaching how to audit AI (the “why” and the “how”). The technology has finally arrived to save the nursing profession from the screen; our task now is to ensure it remains a servant to the human element of care, rather than its replacement.
References & Citations
- Epic Systems Corp. (2026). Winter 2026 Release Notes: Art, Penny, and Emmie Integration Guides.
- athenahealth Research. (2026). The AI-Native Encounter: Impact on Ambulatory Same-Day Closure Rates.
- HIMSS. (2025). Annual State of Healthcare AI: Transitioning to Agentic Models.
- American Nurses Association (ANA). (2024). Position Statement on the Ethical Use of Artificial Intelligence in Nursing Practice.
- Digital Health News. (2026). Epic vs. Athena: The Battle for the Ambient Scribe Market.
- Journal of Nursing Informatics. (2025). Quantifying the ‘Pajama Time’ Reduction: A Multi-Center Study of Ambient Scribing.
- Becker’s Hospital Review. (2026). The ROI of AI: Why Hospitals are Betting on Agentic Models.