By: Jude Chartier RN / AI Nurse Hub
Date: January 26, 2026
Abstract As healthcare systems grapple with increasing patient acuity and a diminishing nursing workforce, the integration of Artificial Intelligence (AI) presents a transformative opportunity to enhance patient safety and clinician well-being. This article explores the transition from traditional, reactive nursing models to proactive, AI-augmented strategies. By addressing the “documentation tax,” enhancing early warning systems, and optimizing operational workflows through predictive analytics, AI serves as a critical socio-technical safeguard. However, successful implementation requires addressing inherent clinician skepticism, particularly regarding “automation bias” and the “replacement narrative.” This paper argues that AI, when framed as “Augmented Intelligence” with a “Human-in-the-Loop” ethical framework, does not replace the nurse but rather empowers the clinician to return to high-touch, patient-centered care, ultimately redefining the professional identity of the nurse in the digital age.
Introduction: The Imperative for Change
In the high-stakes environment of modern healthcare, the margin for error is razor-thin. While clinicians demonstrate immense dedication, the systems they navigate are fraught with complexity; medical errors currently rank as the third leading cause of death in the United States, underscoring a critical need for structural support (Makary & Daniel, 2016). For the frontline nurse, these statistics are not just abstract data points; they represent the cumulative toll of “cognitive overload”—a state where the volume of incoming information exceeds the brain’s processing capacity. This overload is exacerbated by chronic fatigue and a documentation burden that has increasingly pulled the clinician away from the bedside and into a fragmented world of screens and alerts.
The traditional “Swiss Cheese Model” of accident causation—where multiple layers of defense must fail for an error to reach a patient—is being challenged by the sheer speed and complexity of acute care. In this model, the “holes” in the cheese represent latent system weaknesses such as staffing shortages or communication breakdowns. Artificial Intelligence (AI) is emerging as a dynamic, self-healing layer in this model. It acts as a socio-technical safeguard that can transition healthcare from reactive crisis management to a proactive “zero harm” strategy (Robert, 2019). By identifying patterns in the “noise” of modern telemetry and Electronic Health Records (EHRs), AI provides a persistent, objective lens that complements human intuition, catching subtle errors before they propagate through the system.
Addressing the Hesitation: Navigating the “Digital Divide”
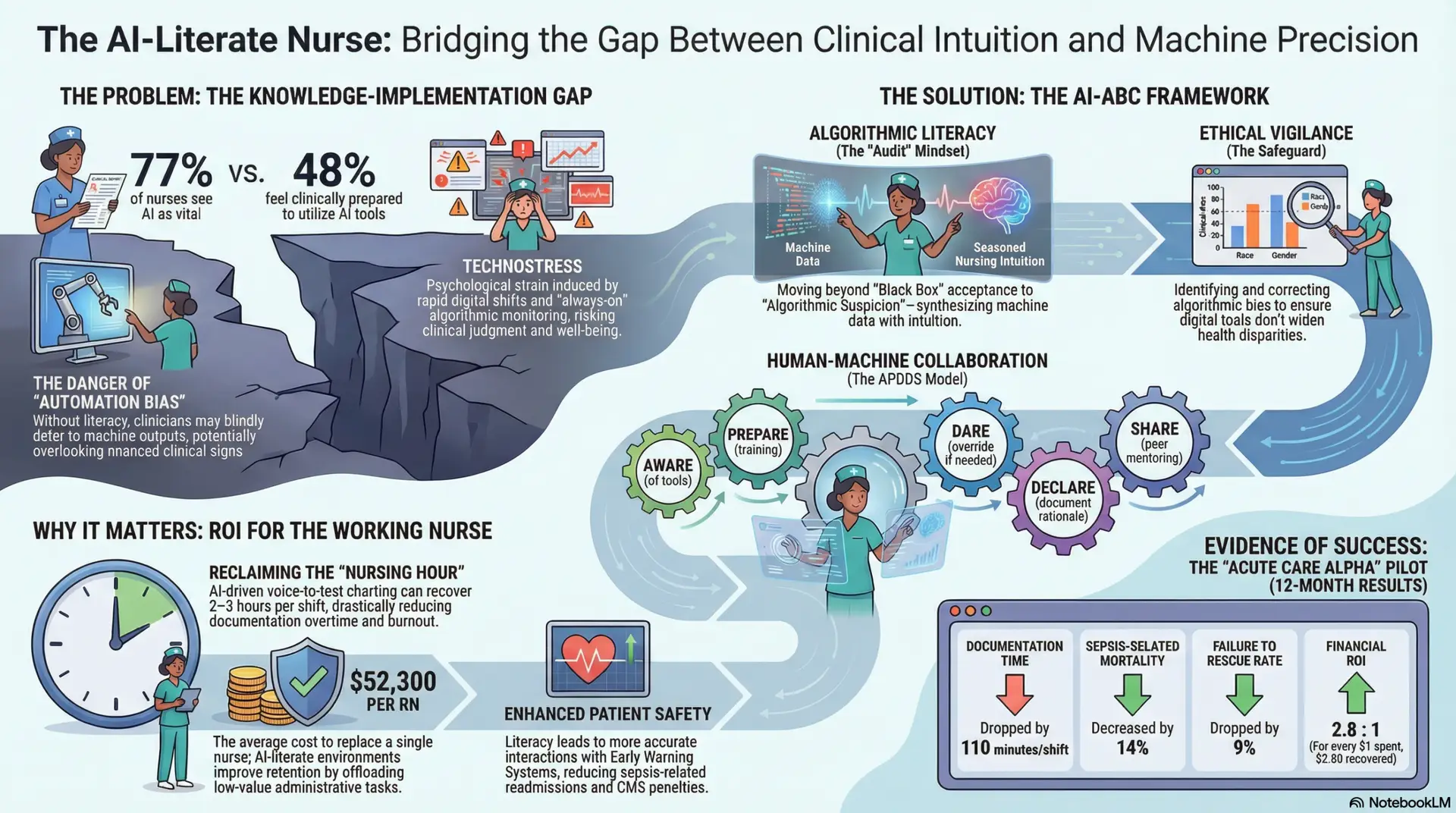
Before embracing a technological future, it is essential to acknowledge the valid reluctance felt by many staff nurses. Skepticism often stems from two primary fears: the “replacement narrative” and the “black box” concern. Nurses may worry that AI will automate their roles or that reliance on algorithms will erode the “clinical gut feeling” developed through decades of direct patient interaction. Furthermore, the history of EHR implementation—which many clinicians feel was designed for billing rather than bedside care—has created a “once bitten, twice shy” mentality toward new software.
The Billing-Centric Legacy vs. Clinician-Centric AI To address this, leaders must distinguish AI from the legacy systems of the past. Traditional EHRs required nurses to adapt their workflows to the computer; modern AI is designed to adapt to the nurse.
Example: The Automation Bias Scenario Consider a nurse who receives an AI-generated alert suggesting a low risk of falls for a patient. If that nurse observes the patient is actually confused, impulsive, and unsteady, they may experience “automation bias”—the tendency to trust the machine over their own physical assessment. To overcome this, healthcare leaders must emphasize that AI is an advisor, not a decider. The shift to AI is fundamentally different from previous IT rollouts; it is designed to be “Augmented Intelligence.” By embracing these tools, nurses are not surrendering their autonomy; they are gaining a digital ally that handles data-heavy tasks, effectively protecting their license and their patients from the limitations of human vigilance.
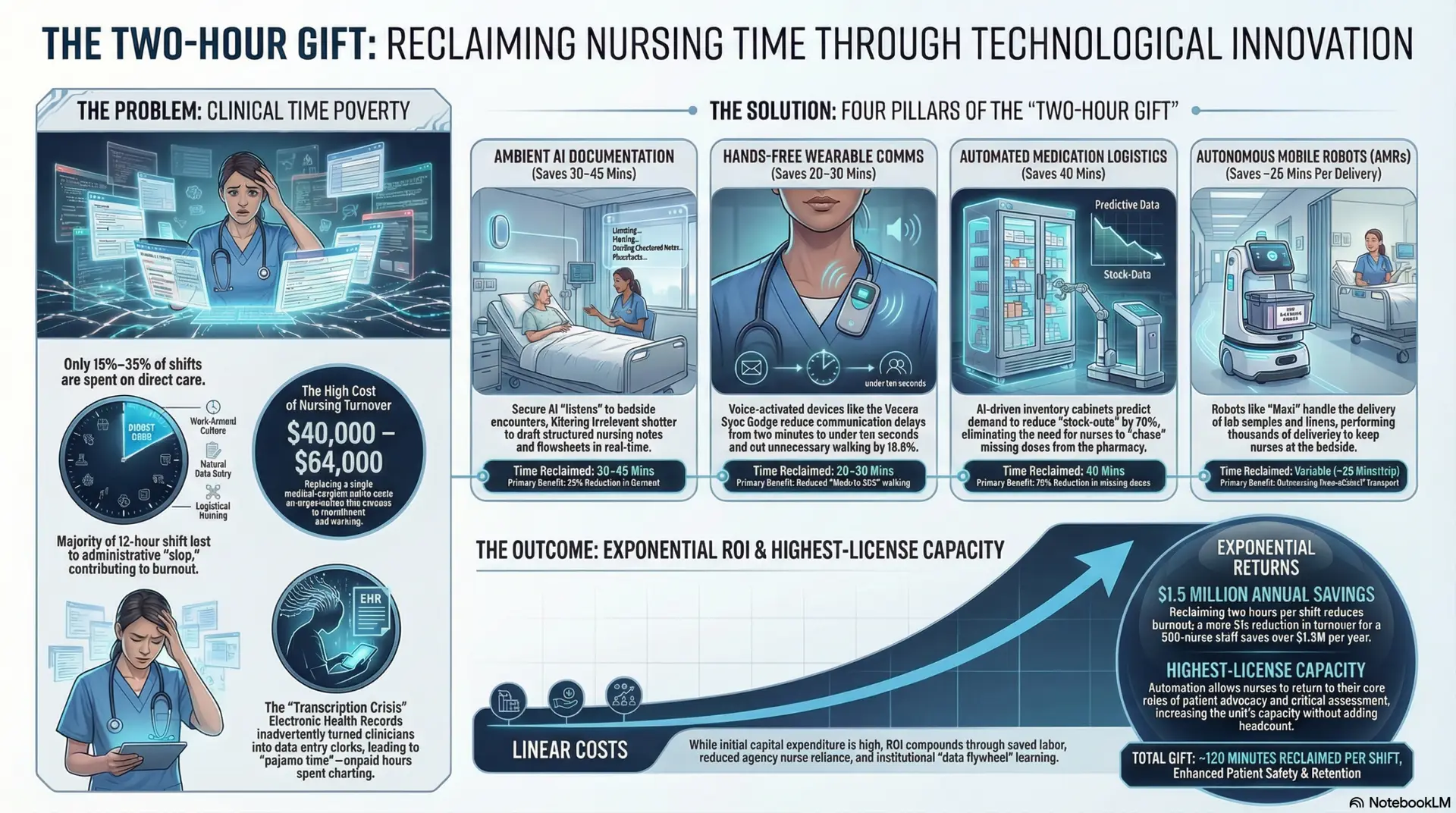
Eliminating the “Documentation Tax”: Returning to the Bedside
Perhaps the greatest advantage AI offers the nursing profession is the mitigation of the “documentation tax.” Current estimates suggest that nurses spend up to 35% of their shift on data entry, leading to “pajama time”—working on charts long after a shift has ended—and significant moral distress (Topol, 2019). This “screen time” is more than just a nuisance; it represents a loss of the “clinical gaze,” the ability of the nurse to observe subtle changes in a patient’s demeanor, color, or breathing that a computer cannot see.
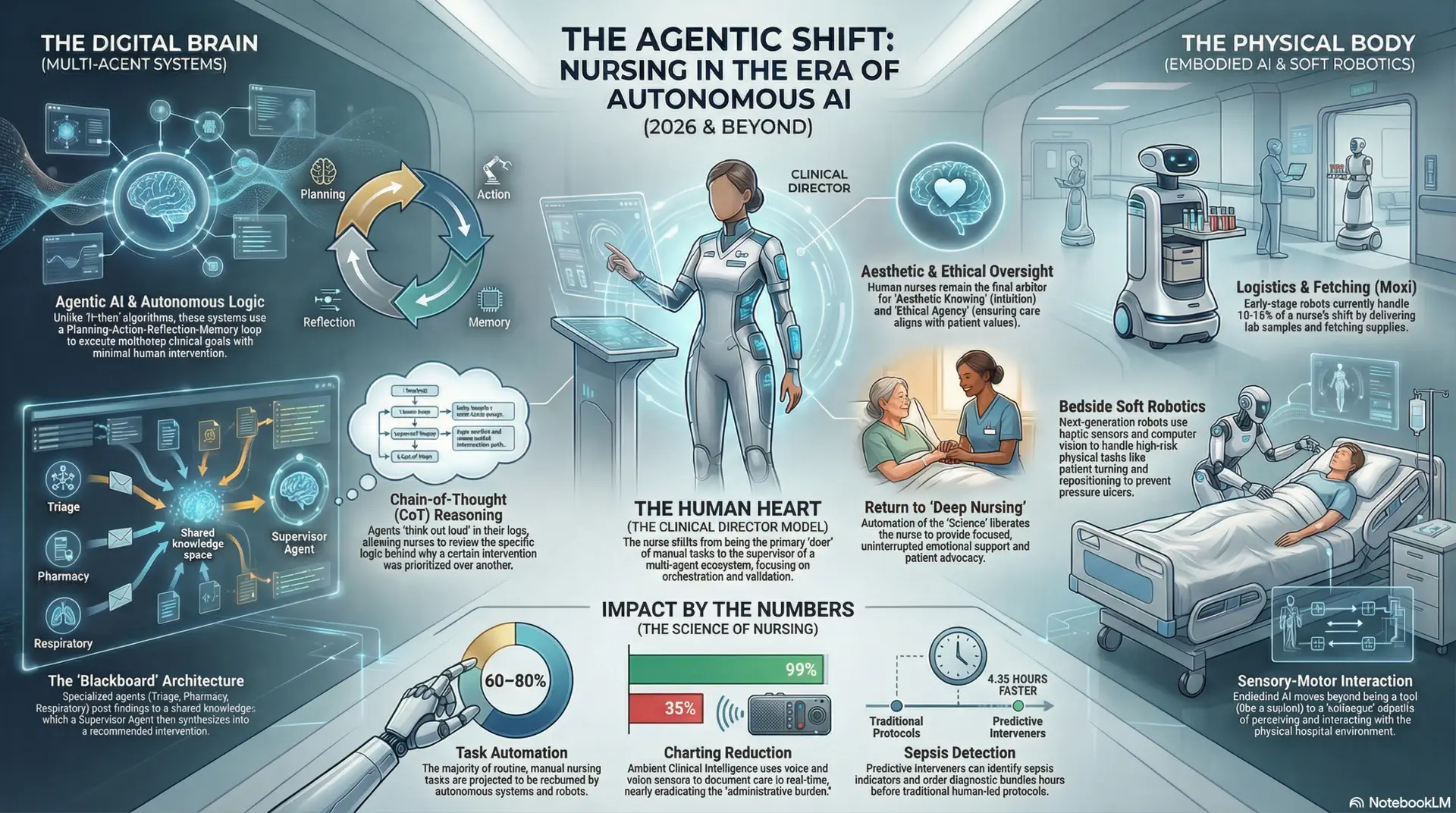
By utilizing Natural Language Processing (NLP) and Ambient Clinical Intelligence (ACI)—technologies that use strategic microphones and AI to understand context during a patient encounter—clinicians can automate up to 50% of routine documentation through seamless, background transcription (Topol, 2019).
Illustration: The AI Scribe in Acute Care Imagine an ICU nurse performing an admission assessment for a critically ill patient. Traditionally, the nurse must juggle life-saving interventions with the need to document dozens of fields in the EHR, often leading to delayed or “copy-paste” charting. With ACI, the nurse can simply speak their assessment findings as they work: “Pupils are equal and reactive; lungs show diminished breath sounds in the bases; skin is cool and clammy.” The AI automatically populates the appropriate flowsheet in real-time. When the burden of the screen is removed, the “therapeutic relationship” is re-established. AI allows the nurse to look the patient in the eye rather than looking at a keyboard, returning the profession to its high-touch, compassionate roots.
The Safety Net: Advanced Early Warning Systems
The value of AI extends beyond simple administrative relief; the data captured through these streamlined workflows feeds into a safety net that never tires. Human vigilance is a finite resource, subject to the physiological limits of a twelve-hour shift. AI-driven Early Warning Systems (EWS) are now capable of analyzing thousands of data points—vital signs, lab results, and even the sentiment of nursing notes—to predict clinical deterioration or sepsis hours before physical symptoms become overt.
Research by Cho et al. (2020) demonstrates that AI-based models show significantly higher sensitivity in detecting patient decline than traditional “modified” EWS scores.
The Predictive Horizon: While a traditional EWS might only trigger once a patient’s heart rate exceeds a static threshold, an AI model identifies the “velocity” of change. It sees the subtle, upward trend in heart rate combined with a slight drop in urine output and a rising lactate level—triggering an alert while the patient is still compensated.
By providing intelligent filtering, these systems also address “alarm fatigue,” a dangerous phenomenon where nurses become desensitized to the constant ringing of monitors. Rather than alarming for every individual outlier, the AI only notifies the nurse when a constellation of factors indicates true risk. For the novice nurse, this provides a critical layer of support, bridging the “experience gap” with real-time, evidence-based suggestions that serve as a professional safety harness (O’Connor et al., 2023).
Systemic Excellence and Operational Stability
For nursing leaders and hospital administration, AI offers a macro-view of facility health that was previously impossible. “Digital Twins”—virtual replicas of hospital workflows—and machine learning models can now predict ward-level infection outbreaks by detecting subtle patterns in environmental and clinical data (Buchanan et al., 2021).
Example: Pathogen Surveillance and Cost Avoidance An AI system might notice that three patients on different ends of a surgical floor have developed similar low-grade fevers. It cross-references their charts and identifies that all three were treated using the same mobile ultrasound machine that wasn’t properly logged for cleaning. This allows for targeted interventions before a single case of a hospital-acquired infection (HAI) becomes a facility-wide outbreak. The cost-saving implications are profound; avoiding a single HAI can save a hospital tens of thousands of dollars in non-reimbursable care costs, providing a clear ROI for AI investment.
Furthermore, AI optimizes staffing through “Dynamic Acuity Modeling.” Rather than staffing based on simple census numbers (e.g., a blunt 1:5 ratio), predictive models can align nursing resources with the actual intensity of care required. If the AI identifies that three patients in a 30-bed unit are at high risk for a “code blue” or significant hemorrhage within the next six hours, it can recommend shifting an extra RN to that unit immediately. This creates a more equitable workload, reducing the moral injury that occurs when nurses feel they cannot provide safe care due to inadequate staffing.
The Ethical Mandate: Human-in-the-Loop
The integration of AI requires a robust ethical framework centered on the “Human-in-the-Loop” (HITL) principle. It is a fundamental tenet of nursing informatics that AI outputs remain clinical suggestions, never mandates. The professional autonomy and accountability of the nurse are paramount; AI provides the evidence, but the nurse provides the context and the final decision (Risling & Low, 2019). Nurses must remain the primary advocates for their patients, using AI as a tool to support, rather than dictate, that advocacy.
To prevent “automation bias,” nursing education must evolve to include “Digital Health Literacy.” Hospital leaders must prioritize “Explainable AI” (XAI). It is not enough for an algorithm to say a patient is “high risk.” The system must show its work: “Alert: High Sepsis Risk (82%) based on 10% increase in WBC, new-onset tachycardia, and history of immunosuppression.” When a nurse understands the logic behind an alert, they are empowered, not bypassed. This transparency builds the trust necessary for true clinical adoption.
Conclusion: A Cultural Evolution
The transition to AI-integrated nursing represents more than a technological upgrade; it is a cultural evolution that requires leadership to invest deeply in the professional development of the nursing workforce. For the staff nurse, it is a shield against error and burnout. For the administrator, it is a tool for operational excellence, fiscal responsibility, and patient safety. As we move forward, the goal is clear: to use the power of data to return the nurse to the bedside. By embracing AI, we are not moving away from the “human” in healthcare—we are protecting it, ensuring that nurses have the cognitive space and time to provide the compassionate care that remains the heart of the profession.
References
Buchanan, C., Howitt, M. L., Wilson, R., Booth, R. G., Risling, T., & Bamford, M. (2021). Predicted influences of artificial intelligence on nursing education: Scoping review. JMIR Nursing, 4(1), e23933. https://doi.org/10.2196/23933
Cho, K. J., Kwon, O., Kwon, J. M., Lee, Y., Park, H., Jeon, K. H., Kim, K. H., Park, J., & Oh, B. H. (2020). Detecting patient deterioration using artificial intelligence in a rapid response system. Critical Care Medicine, 48(4), e285–e289. https://www.google.com/search?q=https://doi.org/10.1097/CCM.0000000000004236
Makary, M. A., & Daniel, M. (2016). Medical error—the third leading cause of death in the US. BMJ, i2139. https://www.google.com/search?q=https://doi.org/10.1136/bmj.i2139
O’Connor, S., Cho, I. T., Dligach, D., Hu, Z., Moen, A., Peltonen, L. M., … & Topaz, M. (2023). Artificial intelligence in nursing: Priorities and opportunities from an international invitational forum of the 2022 International Medical Informatics Association (IMIA) Nursing Informatics (NI) Congress. International Journal of Medical Informatics, 171, 104958.
Risling, T., & Low, C. (2019). A digital practice advocacy framework: Nursing education and the nursing role in a digital healthcare future. Journal of Nursing Education and Practice, 9(6), 115-121.
Robert, N. (2019). How artificial intelligence is changing nursing. Nursing Management, 50(9), 30-39. https://doi.org/10.1097/01.NUMA.0000578988.56622.21
Topol, E. J. (2019). High-performance medicine: The convergence of human and artificial intelligence. Nature Medicine, 25(1), 44-56. https://doi.org/10.1038/s41591-018-0300-7