By: Jude Chartier RN / AI Nurse Hub
Date: February 5, 2026
Abstract
The nursing profession is currently navigating a pivotal transition from manual data entry to high-level clinical oversight. As healthcare systems grapple with unprecedented levels of clinician burnout and fiscal constraints, Artificial Intelligence (AI) has emerged as a dual-purpose solution: a tool for improving staff nurse quality of life and a driver of institutional Return on Investment (ROI). This article explores four critical AI domains—ambient intelligence, predictive analytics, computer vision, and generative literacy—while projecting the future of autonomous robotic integration. By automating administrative burdens and predicting clinical deterioration, AI enables nurses to return to the bedside, simultaneously reducing turnover costs, mitigating litigation risks, and improving patient outcomes.
Introduction: The Evolution from Data Entry to Clinical Pilot
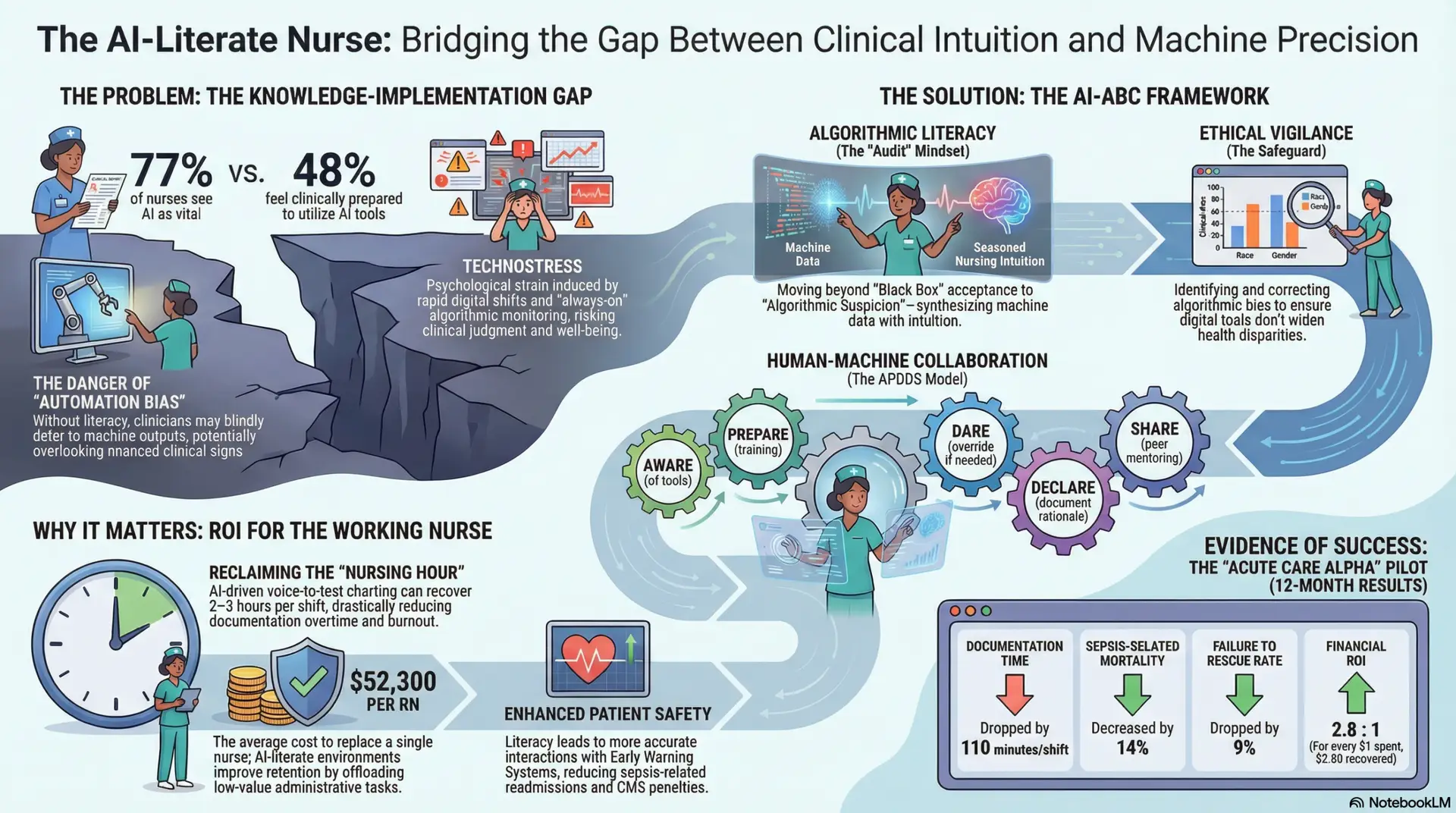
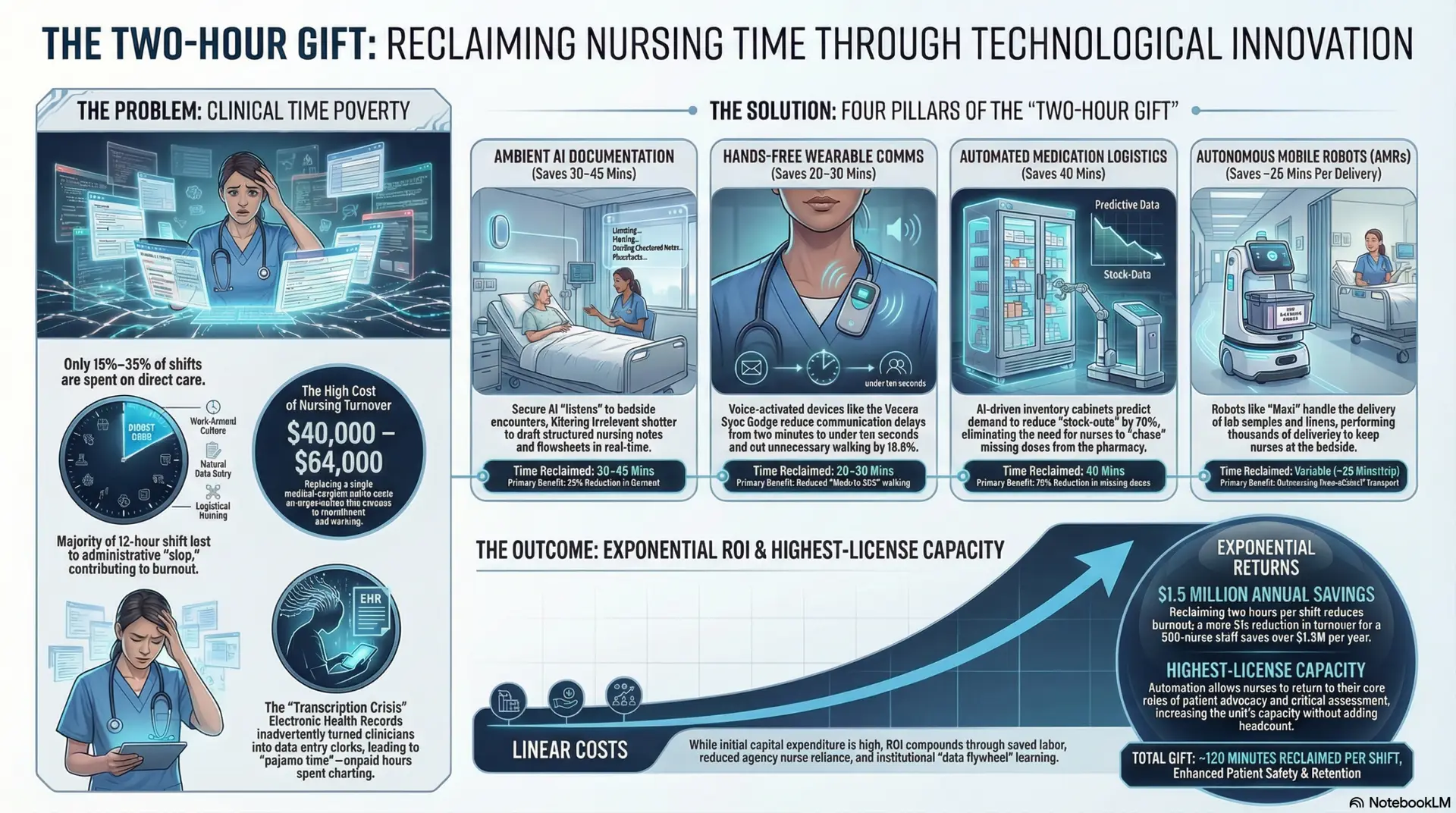
For decades, the nursing profession has been burdened by the “documentation tax”—a phenomenon where nurses spend up to 35% of their shift interacting with Electronic Health Records (EHR) rather than patients. This administrative load, often criticized as “clerical creep,” is a primary driver of documentation burnout, which directly correlates with nurse turnover, moral injury, and medical errors. Historically, the EHR was designed for billing rather than bedside care, forcing nurses into the role of data transcriptionists.
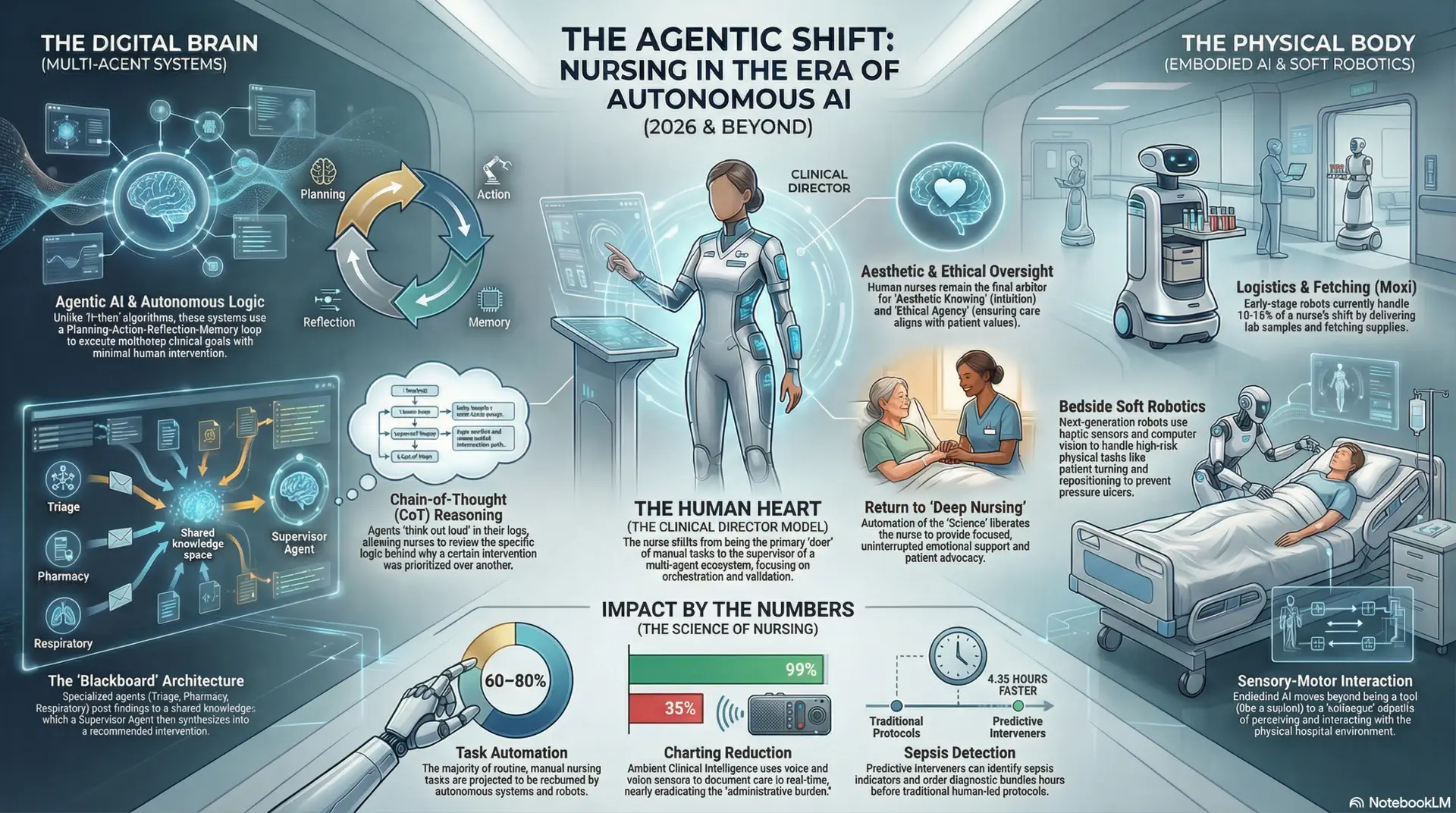
However, the reality of 2026 marks a paradigm shift. AI is no longer a peripheral technology but a core clinical partner. The role of the nurse is evolving from a data gatherer to an AI Pilot, responsible for interpreting, validating, and acting upon high-level machine insights. For administrators, this shift represents a significant ROI opportunity. By stabilizing the workforce through reduced burnout and maximizing clinical efficiency, institutions can transition from a defensive “crisis staffing” posture to a strategic “optimized care” model.
Ambient Clinical Intelligence: The End of the “Keyboard Barrier”
The most immediate relief for the staff nurse comes from Ambient Clinical Intelligence (ACI). These systems utilize advanced Natural Language Processing (NLP) and multi-modal sensors to listen to nurse-patient interactions, distinguishing between conversational rapport and clinical data. During a post-operative assessment, for example, the ACI system can capture the patient’s pain level, the status of the surgical site, and the nurse’s verbal instructions on incentive spirometry, automatically populating the structured fields of the EHR in real-time.
From a scholarly perspective, the benefits are quantifiable. A 2025 randomized clinical trial published in JAMA Network Open demonstrated that ambient AI tools reduced documentation time by over 15%, recouping multiple hours of clinical time per week for staff (Pearlman et al., 2025). This “found time” is critical; it allows for the “human-to-human” connection that defines high-quality nursing care. For administration, the ROI is twofold. First, it significantly reduces “pajama time”—the practice of nurses staying after their shift to finish charting—which lowers overtime costs and burnout-related turnover. Second, ACI improves coding accuracy and document completeness, ensuring that the hospital is appropriately reimbursed for the acuity of the care provided.
However, this shift requires a new nursing skill: Auditory Validation. Nurses must move from manual entry to an auditing role, ensuring that AI-generated summaries accurately reflect patient safety concerns and clinical nuances (Olson et al., 2025). This transition requires institutional investment in “AI Literacy” training to ensure staff can confidently supervise the machine’s output.
Predictive Analytics & Digital Twins: Catching the “Crash”
While ACI handles the past (documentation), predictive analytics focuses on the future. Modern hospitals utilize “Digital Twins”—virtual replicas of patients built from a continuous stream of real-time physiological data, laboratory results, and historical records. These systems use machine learning to simulate potential outcomes, identifying subtle patterns—such as a specific combination of heart rate variability and lactic acid trends—that are invisible to even the most experienced human eye.
Meta-analyses show that these AI-powered early warning models significantly reduce in-hospital and 30-day mortality rates by predicting sepsis or respiratory failure hours before traditional Early Warning Scores (EWS) would trigger (Yuan et al., 2025). For the staff nurse, this means a shift from reactive “rescue” mode to proactive clinical management. Instead of responding to a “Code Blue,” the nurse is alerted to a “Probable Sepsis Risk” three hours in advance, allowing for the initiation of fluid resuscitation and antibiotics before the patient reaches a critical state.
For the hospital administrator, the financial ROI is substantial. Reducing a single case of hospital-acquired sepsis can save an institution tens of thousands of dollars in non-reimbursable care costs and potential litigation. Furthermore, these tools help in bed management and resource allocation, ensuring that ICU beds are available for those who truly need them. Success in this area relies on the nurse’s ability to utilize Clinical Decision Support (CDS) systems while maintaining the clinical intuition to “overrule” the data when the bedside assessment contradicts the algorithm (Elhaddad & Hamam, 2024).
Computer Vision & Smart Rooms: The Invisible Watcher
The integration of Computer Vision (CV) into “Smart Rooms” represents a monumental leap in patient safety. Wall-mounted sensors, utilizing edge computing to maintain privacy, monitor patient movement 24/7. These systems can detect “pre-event” behaviors, such as a patient dangling their legs over the bedside or attempting to stand without assistance.
Recent research demonstrates that AI-based monitoring systems result in a statistically significant reduction in accidental falls, with an incidence rate ratio of 0.21 compared to unmonitored environments (Frontiers in Digital Health, 2025). For nurses, this technology mitigates the constant anxiety of “fall risk” patients, especially during night shifts or when staffing ratios are stretched. CV can also monitor skin integrity by tracking how long a patient has been in a specific position, automatically alerting the nurse if a “turn” is overdue, thereby preventing costly and painful pressure ulcers.
From an administrative standpoint, the ROI is seen in the drastic reduction of “constant observer” or “sitter” costs. Historically, hospitals have spent millions annually hiring staff to sit in rooms with high-risk patients. CV allows one technician to monitor dozens of rooms with AI-assisted highlighting of high-risk movements. This not only saves on labor costs but also improves the quality of care by providing a more reliable, “always-on” safety net (Seibert et al., 2025).
The Future Projection: Autonomous Caregivers and Direct Summons
Perhaps the most transformative projection for the near future is the direct integration of Smart Rooms with autonomous robotic caregivers. Current trends suggest that by the end of the decade, AI-monitored rooms will be able to distinguish between clinical needs and “trivial” or “hospitality” requests.
In this future scenario, the “Smart Room” acts as a triage center. If a patient requests a fresh blanket or a cup of ice via a voice assistant, the system verifies the request against the patient’s diet and safety orders. If the request is non-clinical, the system bypasses the nurse’s workstation and the central call-light system entirely, automatically summoning an autonomous robotic caregiver (such as a delivery bot or a mobile robotic arm) to fulfill the request.
This “triage of tasks” represents a monumental shift in nursing workflow. By automating the fulfillment of non-clinical needs, nurses are freed from the constant interruptions of “call-light fatigue,” which studies have shown can occur hundreds of times per shift. For administration, this directly impacts HCAHPS scores—a key metric for Medicare reimbursement—by ensuring near-instantaneous response times for patient comfort requests. More importantly, it allows the highly-compensated, highly-trained nursing staff to focus exclusively on “top-of-license” clinical tasks, such as titration of vasopressors, wound care, and emotional support for families.
Generative AI for Health Literacy: The Translation Bridge
Generative AI (GenAI) through Large Language Models (LLMs) is revolutionizing the “discharge bridge.” One of the leading causes of readmission is a patient’s failure to understand their post-hospital care instructions. Nurses are now using GenAI to instantly translate complex, jargon-heavy discharge summaries into any language, adjusted for the patient’s specific reading level or even converted into a pictorial guide for those with cognitive impairments.
Generative AI is identified as a critical solution for improving health literacy and clinical safety by providing accessible, tailored information (Frontiers in Digital Health, 2025). For the staff nurse, this eliminates the time-consuming process of waiting for a phone-based translator or manually simplifying medical terminology. For the administrator, improved health literacy leads to lower 30-day readmission rates, avoiding the heavy financial penalties imposed by CMS. However, nurses must maintain “AI Literacy” to act as the final check against potential “hallucinations”—where the AI might provide confidently wrong medical advice—ensuring that the generated instructions are clinically safe and culturally sensitive (Rodger et al., 2025).
Conclusion: The “Human-in-the-Loop” as the Ultimate ROI
As we look toward the fully integrated hospital of the future, the value of the nurse is not diminished but elevated. AI can process vast quantities of data and automate repetitive physical tasks, but it cannot provide the advocacy, empathy, or ethical judgment required in complex human care. AI cannot navigate the nuance of a difficult end-of-life conversation, nor can it provide the intuitive “gut feeling” that a patient “just doesn’t look right” despite stable vitals.
The nurse remains the essential “Human-in-the-Loop” (HITL). For administrators, the ultimate ROI of AI is not the replacement of human staff, but the optimization of the nursing workforce. By investing in these technologies, hospitals create an environment where the most skilled clinicians are no longer clerical workers, but “Clinical Pilots” who have the time and the data to practice the true art of healing. In 2026, the competitive advantage of a healthcare institution will not be measured by its software alone, but by how effectively that software empowers its nurses to be human.
References
Elhaddad, M., & Hamam, A. (2024). Artificial intelligence in nursing practice: Decisional support, clinical integration, and future directions. Online Journal of Issues in Nursing (OJIN), 30(2). https://www.google.com/search?q=https://doi.org/10.3912/OJIN.Vol30No02Man01
Frontiers in Digital Health. (2025). Prevention of falls in hospitalized patients—evaluation of the effectiveness of a monitoring system developed with artificial intelligence. Frontiers in Digital Health, 7. https://www.google.com/search?q=https://doi.org/10.3389/fdgth.2025.1548209
Olson, K., Meeker, D., & Shah, S. (2025). Use of ambient AI scribes to reduce administrative burden and professional burnout. JAMA Network Open, 8(10), e258614. https://www.google.com/search?q=https://doi.org/10.1001/jamanetworkopen.2025.258614
Pearlman, K., Wan, W., & Laiteerapong, N. (2025). Use of an AI scribe and electronic health record efficiency. JAMA Network Open, 8(10), e251904. https://www.google.com/search?q=https://doi.org/10.1001/jamanetworkopen.2025.1904
Rodger, D., Mann, S. P., & Savulescu, J. (2025). Generative AI in healthcare education: How AI literacy gaps could compromise learning and patient safety. Nurse Education in Practice, 87. https://www.google.com/search?q=https://doi.org/10.1016/j.nepr.2025.104461
Seibert, K., et al. (2025). ETHICS of AI adoption and deployment in health care: Progress, challenges, and next steps. JMIR AI, 4(1), e67626. https://www.google.com/search?q=https://doi.org/10.2196/67626
Yuan, S. X., & Wu, C. D. (2025). AI-powered early warning systems for clinical deterioration significantly improve patient outcomes: A meta-analysis. BMC Medical Informatics and Decision Making, 25(1), 203.